The Smartphone Minerals War That Destroyed Congo's Health System — Just in Time for Ebola
Rwanda’s mineral extraction, America’s aid cuts, and the most money-driven conflict one epidemiologist has ever seen.

300,000 is not a headline.
Eighty people have died of Ebola in eastern Congo. That made global headlines and triggered a WHO Public Health Emergency of International Concern.
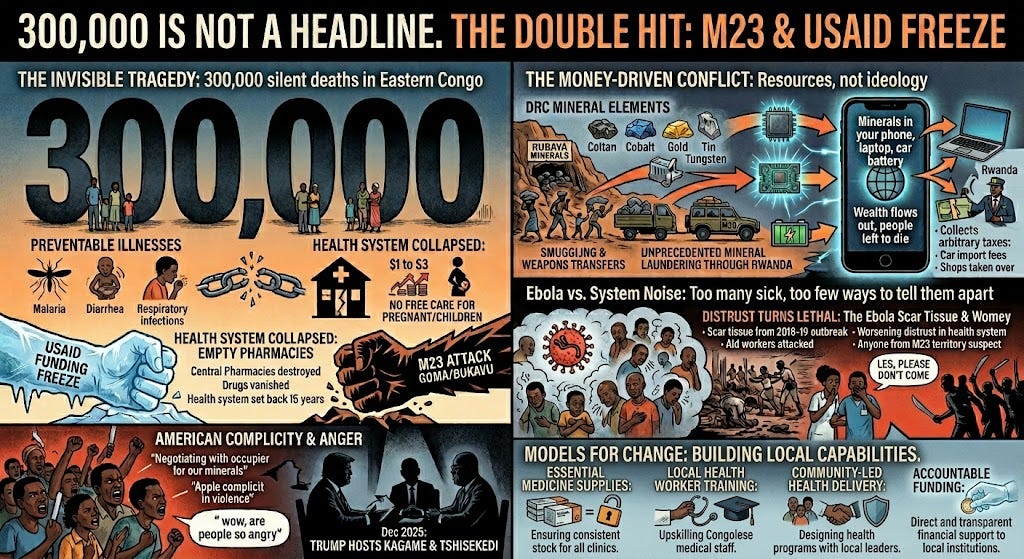
Here is a number that did not make headlines: 300,000.
That is the estimated excess death toll in North and South Kivu since February 2025 — not from Ebola, not from bullets, but from a health system that stopped working. The cause of death is malaria. Diarrhea. Respiratory infections. The things that kill when clinics have no drugs to give.
Les Roberts is an epidemiologist and professor emeritus at Columbia University who has spent 40 months working in Congo since 1994. He has run more than 50 mortality surveys in conflict zones. His team, working with a local NGO called Rebuild Hope for Africa, surveyed 900 households across 60 randomly selected clusters in both provinces in August and September last year. The finding? Mortality doubled after February 2025. (He couldn’t share more because his paper is currently under review at BMJ Global Health.) Mortality rates have not come back down.
“The doubling of mortality was not about violence,” Roberts told me. “Violence was, I don’t know, cause number six or something. It was about malaria and diarrhea and respiratory infections.”
And the timing could not be worse.
M23 and USAID: the double hit.
To understand what happened, you need to understand two things that happened within days of each other.
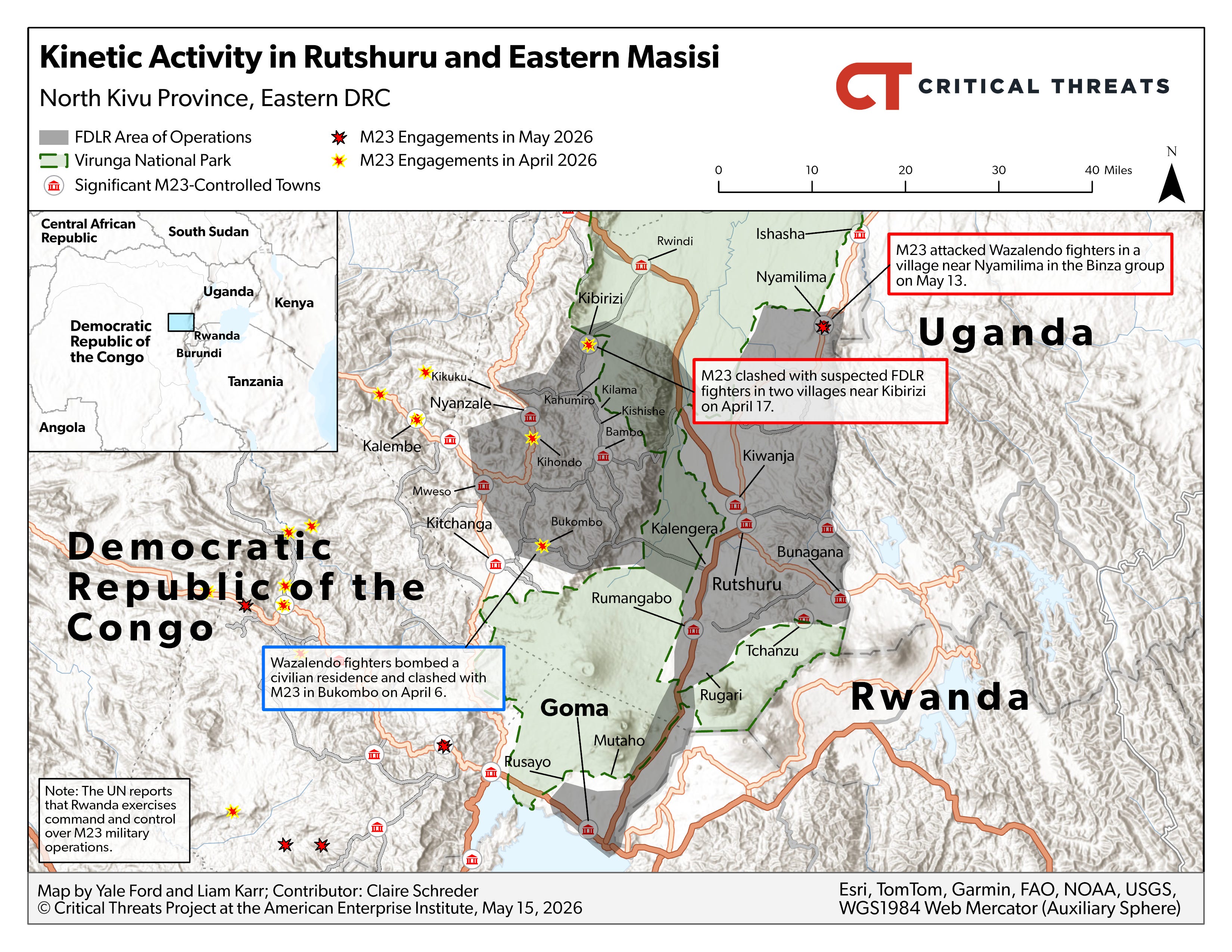
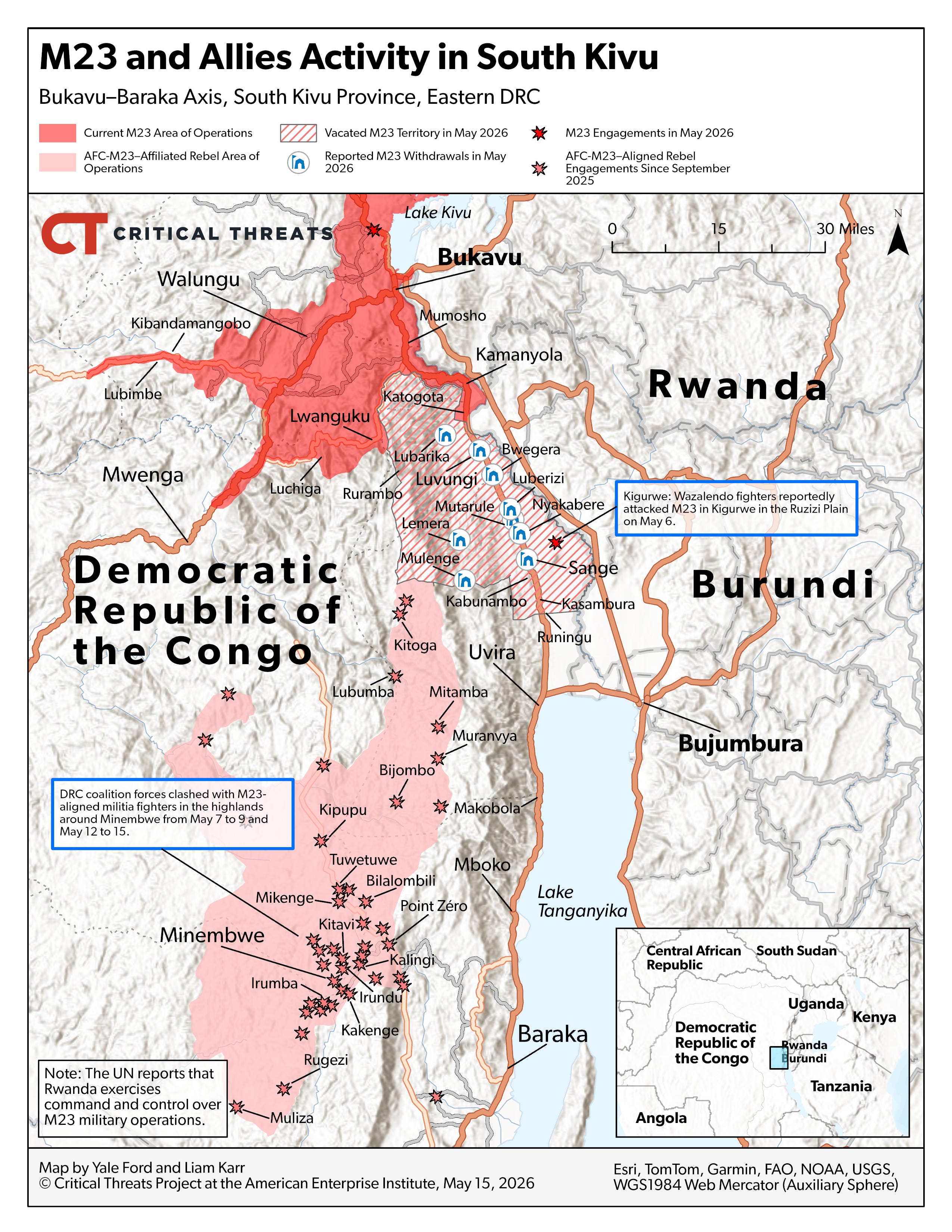
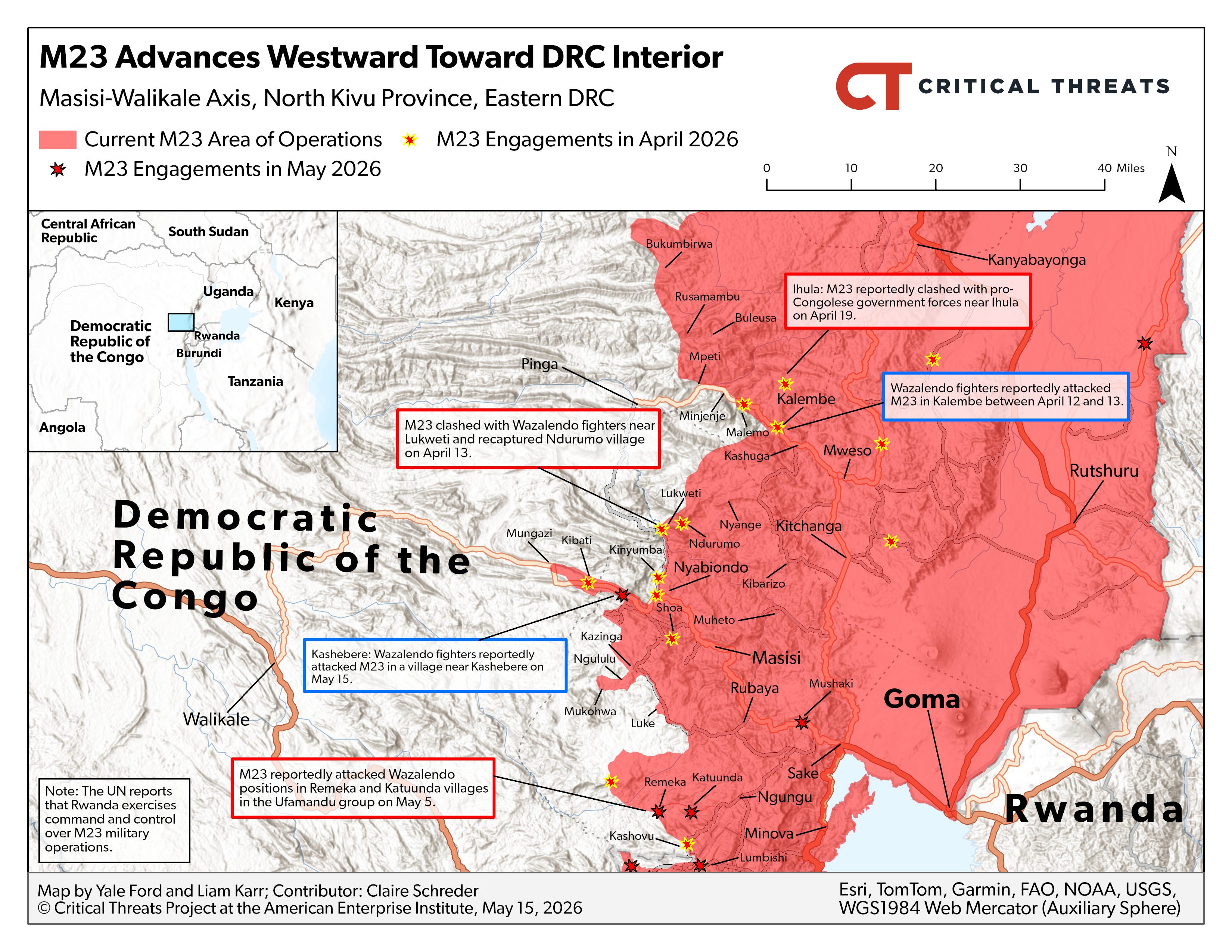
In late January 2025, M23, a rebel group backed by Rwanda, seized Goma, the capital of North Kivu province and the logistics hub for the entire eastern Congo humanitarian operation. Within weeks, they took Bukavu, the capital of South Kivu, too. That same week, the Trump administration froze USAID funding.
“Realize that the M23 takeover and the USAID freeze of money happened at almost the same time, within a week of each other,” Roberts said. “And that’s probably not by chance.”
Roberts believes M23 timed the offensive for the transition. “When the M23 took over Goma back in 2013, Obama was president,” he said. “He called up Paul Kagame the very next day and said, ‘This is unacceptable. We will freeze’ — whatever they had, four hundred million or seven hundred million dollars in aid — ‘if you don’t cut this crap out.’ And the M23 pulled out the next day.”
This time, no call came.
Together, these destroyed the health system through one mechanism: the collapse of the central pharmacies. In North and South Kivu, the Centrales de Distribution Régionale are how medicine reaches rural clinics. USAID had built a system where NGOs funneled drug shipments through these pharmacies. When funding froze, the pharmacies couldn’t function. “Suddenly all these NGOs stopped having their drugs come in,” Roberts said. “The whole system collapsed.”
Clinics that charged one dollar now charge three. Free treatment of pregnant women and children under five disappeared. “You had to go and get the drug on your own,” Roberts said. “And it wasn’t around, ‘cause the logistics systems disappeared, and people couldn’t afford it.”
“In one year we have literally moved the health system back ten or fifteen years of development,” he told me.
The most money-driven conflict he has ever seen.
This war is not primarily about ideology or ethnicity. It is about extraction.
“I’ve never seen such a money-driven conflict as I saw there,” Roberts said. “Rwanda’s overall motivation is resource and financial.”
According to UN investigators, some 4,000 Rwandan troops are fighting inside Congo. Rwanda denies it. But UN experts have documented Rwanda’s command and control over M23, weapons transfers, and mineral smuggling at what the investigators called “unprecedented levels”.
The prize is minerals, and many of them are in your smartphone.
Eastern Congo holds over 40% of the world’s coltan, from which tantalum is extracted for the capacitors that regulate power in every phone. Tin from the region is used in the solder that holds circuit boards together. Gold goes into the connectors. Tungsten is in the vibration motor. The Rubaya mine in North Kivu alone accounts for about 15% of global coltan output. M23 took full control of it in April 2024 and collects an estimated $800,000 a month taxing coltan, tin, tungsten, and manganese. The DRC also produces 73% of the world’s cobalt — the key ingredient in the lithium-ion batteries that power phones, laptops, and electric vehicles.
“Gold and diamonds are the big value items,” Roberts told me. “But they might not be the main things that have effect. There’s other things like columbite-tantalite and other rare earth minerals that are pretty interwoven with this.”
The minerals are smuggled into Rwanda and laundered through its export system. Rwanda earned $1.1 billion in 2023 from minerals commonly mined in eastern Congo — a 43% jump from the previous year — despite having little domestic production. Rwandan law allows imports to be relabeled as Rwandan with 30% value addition. The gap is Congolese coltan entering the global supply chain as Rwandan product.
But the extraction goes far beyond mining. Roberts described a system of total economic control. Rwanda shut all M23-controlled border crossings with Uganda “so that Rwanda would be the one importing anything coming in and anything going out,” he said. M23 collects car importation fees on the Rwandan side and issues receipts labeled “for agricultural produce,” so there’s never a record. “All the shops along the Rwandan border have been taken over by Rwandans and have good products, and there’s very little products in the older ones two miles in across the border,” he said.
“Dozens of households, when we asked them, ‘Is there anything else you’d like to say?’ would get really agitated and say, ‘We have a right to this land. This land was my grandfather’s,’” Roberts told me. People are being pushed off land for agriculture and mineral activity.
Meanwhile, M23 is spending nothing on health. “They are all about extracting money,” Roberts said. “They are spending nothing, doing nothing to promote the health system.”
Why people are so angry at America.
In December 2025, Trump hosted Kagame and Tshisekedi at the White House to sign a peace deal. He announced that U.S. companies would operate in both countries to extract rare-earth minerals. Tshisekedi had already offered the U.S. access to critical minerals — including the Rubaya tantalum deposit, still under M23 control — in exchange for help defeating the rebels. The peace talks themselves could boost Rwandan processing of Congolese minerals. Fighting has not stopped. To Congolese people, this looks like America negotiating with their occupier to take their minerals.
Roberts has spent 40 months in Congo since 1994. His local staff always wanted him nearby. A white person in the car was protective. Last summer, that flipped.
“Staff were terrified of being out with a white person,” he told me. “Almost always they’d say, ‘Les, Les, please come with me to Beni.’ And now they would say, ‘Les, you can’t come to Beni, man. You will bring hell down on us.’”
“Anyone with a university degree, when they found out I was American, brought it up, and wow, were people so angry,” he said. Congo’s president has accused Apple of being complicit in the violence by using Rwandan-sourced coltan. “The notion that the US president was negotiating with Paul Kagame to get those minerals. I don’t have an example of what I could possibly bring up in the United States that would be so outrage-inducing.”
Too many sick, too few ways to tell them apart.
This is where the Ebola outbreak meets the health system collapse.
I’ve written about the clinical challenge: early Ebola looks like malaria, typhoid, labor. In a functioning system, clinicians can test, triage, and isolate. They can tell the signal from the noise. In a collapsed system, the noise is so loud that the Ebola signal is lost in it.
Before the collapse, there were PPE stockpiles, trained staff, and informal social networks connecting clinicians to the community. “IRC had a pot of money, and they were training people on PPE use and preparation in case there was another hemorrhagic fever outbreak,” Roberts said. “There were all of these things in place, which have very much dissolved. Most of the NGOs have laid off most of their staff.”
The médecins chefs de zones and the people who ran the central pharmacies had relationships that let someone call at midnight and say, “We’re treating seventeen cases and we’re out of PPE — can’t you do something?” “And that person would fix the problem for them,” Roberts said. “I just fear that that social fabric is freaking shattered.”
I asked him to compare this to West Africa in 2014. “The disposition of this population to not trust the health system and not trust clinicians is way higher than we saw in West Africa in 2014,” he said. “For security reasons, for logistic reasons, and for social fabric reasons, we’re in a way, way, way harder context.”
Womey. When distrust turns lethal.
I kept thinking about Womey as Roberts talked.
In September 2014, during the West African Ebola epidemic, eight aid workers were massacred in the village of Womey in southeastern Guinea. They were health workers, journalists, and government officials who had come to educate the community about Ebola. Villagers attacked them with machetes and clubs.
When I worked in Guinea during that outbreak, people told me “Ebola business” was invented to keep politicians in power and aid organizations collecting money. “All that is for me, without me, is against me,” many said.
Roberts is seeing the same dynamics in eastern Congo, but worse. In the north of North Kivu, where the 2018-2019 Ebola outbreak killed 2,299 people, distrust of clinics and NGOs was “way, way, way more negative” than anywhere else his team surveyed. That billion-dollar, heavily militarized response left scar tissue that is still there five to six years later.
“If we don’t do a lot better this time,” Roberts said, “something really bad that was already there is gonna grow more.”
What this means for containment.
Here is the operational picture for anyone trying to respond to the Bundibugyo Ebola outbreak in this region.
Half of North and South Kivu is outside M23’s control, run by Wazalendo militias that Roberts described as “brutal in terms of raping women and stealing food and just living off the population in the most parasitic of ways.” His interviewers knew they would be beaten entering those zones. They went anyway. “Local NGOs can make that decision,” Roberts said. “No way in hell when I was at IRC could IRC ever send interviewers to a place when they knew they were gonna get beaten. No way would MSF ever do that.”
M23 itself would welcome outside health workers, not out of goodwill, but because it’s spending nothing on health. “For NGOs to come is only good to them,” Roberts said. But in the half of the Kivus outside M23 control, any organization entering from M23 territory is immediately suspect.
Roberts was direct about what would work. “If they set up a system so that local clinic workers were replaced by other clinicians, and the locals were free to go out in their community and try to motivate people, it might work well,” he said. “But that is not the United Nations style.”
Despite everything, communities were warm to the local NGO his team worked with. Chiefs thanked them. Households were grateful someone was listening. The path to get in exists, but it requires putting local organizations in front, not behind.
The disaster behind the disaster.
Roberts put the disparity plainly: “How insane that 80 people die of Ebola and it gets front page news, because of essentially the economic and health system collapse that we played a role in, and it gets no attention at all.”
“When things have a short, clear causal pathway or are photogenic, they get covered really well,” he said. “When something like this involves economic and social fabric collapse, it just can’t be talked about.”
The Ebola outbreak matters. It is a rare strain with no vaccine and no treatment. It has crossed a border. WHO was right to declare a PHEIC.
But behind the headlines sits a much larger disaster. A pharmacy system that served millions was destroyed in weeks. A health system was set back fifteen years in twelve months. Three hundred thousand people may have died from conditions that are cheap to treat when the drugs exist, and the clinics work. The minerals from those provinces are in your phone, your laptop, your car battery. The wealth flows out. The people are left to die.
“It is a crazy economically driven war,” Roberts said. “We’re talking 300,000 dead people probably so far, in excess above the baseline.”
The world is watching the Ebola outbreak. Almost no one is watching this.