

Congo’s New Ebola Outbreak Has No Vaccine, No Treatment, and Has Already Crossed a Border
Bundibugyo ebolavirus confirmed in Congo and Uganda. The world has no approved countermeasures for it.



Bundibugyo returns
Africa CDC confirmed today that an Ebola outbreak in eastern Congo has killed at least 65 people. There are 246 suspected cases in Ituri Province. Lab results have identified the virus as Bundibugyo ebolavirus.
Hours later, Uganda’s Ministry of Health confirmed an imported case: a 59-year-old Congolese man admitted to Kibuli Muslim Hospital in Kampala on May 11th with fever, nausea, and respiratory distress. He deteriorated and died in intensive care on May 14th with bleeding symptoms. His body was transported back to Congo that evening. Uganda’s lab confirmed Bundibugyo ebolavirus. Cross-border spread is no longer a theoretical risk. It has happened.
There is no approved vaccine for Bundibugyo. There is no approved treatment. There is no vaccine ready for this species that’s ready for a clinical trial.
This is Congo’s 17th Ebola outbreak. It is the country’s second in less than a year. But the combination of a rare viral species, active armed conflict, a confirmed cross-border case, and an outbreak that reached this size before the world noticed makes it different from the ones that came before.
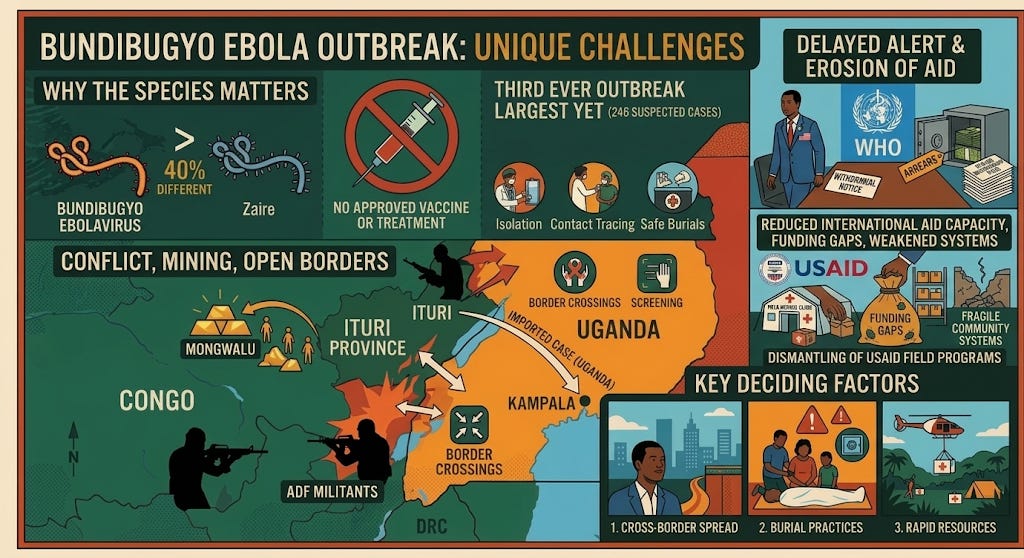
Why the species matters
Bundibugyo ebolavirus has only caused two known outbreaks before this one. The first was 56 cases in Uganda in 2007, in Bundibugyo District, right across the border from where this outbreak is now. The second was 57 cases in Congo in 2012. This would be the third ever, and it is already the largest. Because the virus has appeared so few times, scientists have far less data on how it behaves in human populations than they do for the Zaire species, which has caused dozens of outbreaks over nearly 50 years.
The problem is practical. Over the past decade, the world built Ebola vaccines and treatments: Ervebo, Inmazeb, Ebanga. All of them target the Zaire species. Bundibugyo and Zaire are about 40% different genetically. That is enough that a vaccine for one does not protect against the other. The tools that helped end the 2018-2020 outbreak in this same region, which killed 2,299 people, will not work here.
There are experimental vaccines in the pipeline. Oxford and Moderna are working on a broad vaccine funded by CEPI and the EU that would cover Bundibugyo, Sudan, Zaire, and Marburg. But it is still in early development. Sabin and IAVI have Sudan ebolavirus vaccines in clinical trials. Nothing that targets Bundibugyo is close to being ready. That leaves responders with the basics: finding and isolating sick patients, tracing their contacts, and making sure burials are safe. Ebola spreads through direct contact with the body fluids of a person who is sick or has died. Unsafe burial practices, where family members wash and prepare the body, have been a major driver of past outbreaks.
The case fatality rate for Bundibugyo in past outbreaks has been roughly 36-40%. That is lower than Zaire, which can reach 60-90%. It is still extremely high.
Conflict, mining, and open borders
Ituri Province is more than 1,700 kilometers from the capital, Kinshasa. It sits in one of the hardest places to work in central Africa. ADF militants are active in the area. That limits where health workers can go and makes it harder to track who is sick.
One of the two main outbreak zones, Mongwalu, is a gold-mining town. Workers move in and out constantly. The other, Rwampara, is near Bunia, the largest city in the province. The outbreak sits right along the borders with Uganda and South Sudan. The Kampala case shows the virus had already crossed the border before anyone knew the outbreak was underway. After confirming the case, Uganda activated a national response, deployed screening and surveillance teams at border crossings and transit routes, set up a mobile lab at Bwera Hospital near the western border, and began quarantining all contacts of the deceased patient.
Africa CDC has called an emergency meeting with both countries, WHO, UNICEF, the US CDC, European CDC, MSF, Merck, Moderna, BioNTech, the Gates Foundation, Wellcome Trust, and others. The breadth of that list reflects how seriously the situation is being taken.
Only 20 of the 246 suspected cases have been tested so far. Thirteen came back positive. As testing expands, the confirmed count will rise. Possibly fast.
246 cases before anyone noticed
One detail stands out. It was Africa CDC that publicly declared this outbreak. The Congolese government has not. WHO said today that it received a signal of suspected cases on May 5th and sent a team to Ituri. Initial field tests came back negative. Samples were then sent to INRB, the national lab in Kinshasa, which confirmed Ebola only yesterday. WHO’s global alert network did not discuss the outbreak as recently as the day before that. For suspected cases to reach 246 before the outbreak surfaces to the international community raises a question: how long was this signal missed, or held back?
That gap matters. If community surveillance in Ituri failed to catch it early, that points to weak systems in a province that has seen Ebola before. If the information was known and not shared, that is a different problem.
The erosion of international response capacity makes either answer worse. The dismantling of USAID has already reduced staffing for contact tracing, screening at border crossings, and laboratory capacity in the region. Reporting from South Africa during Uganda’s Ebola response last year found that while systems were still holding, they were visibly weakened. Asked about reduced US funding in Africa, CDC director Jay Bhattacharya said the agency has country offices in both the DRC and Uganda and is "absolutely committed" to providing resources. But CDC provides technical expertise. The contact tracing teams, border screening staff, and laboratory workers that USAID was funding are a different question, and Bhattacharya did not address it. The broader trajectory is not reassuring.
In November 2023, Robert F. Kennedy Jr. told a Children's Health Defense conference that if he had power over NIH, he would redirect it away from infectious-disease research for years: "I'm gonna say to NIH scientists, God bless you all. Thank you for public service. We're going to give infectious disease a break for about eight years." Pathogens do not reciprocate. The research Kennedy wanted to pause is what supports outbreak detection, vaccine development, and pathogen surveillance for exactly this kind of event.
The US and DRC signed a $1.2 billion cooperation agreement earlier this year, $900 million from the US and $300 million from the Congolese government, but it is unclear when that money will begin reaching the ground. In the meantime, the infrastructure it was meant to replace has already been taken apart.
Three things that will decide this
The virus has already crossed into Uganda. The question now is how far it has spread and whether the response can catch up. It is not yet clear how long the patient in Kampala was symptomatic before being admitted, or how many people he had contact with while in the city. Kampala is an international travel hub. Rapid contact tracing will be critical. Three things matter most: whether additional cases surface in Kampala or along the border, whether the body that was transported back to Congo on May 14th leads to further transmission, and whether the emergency coordination translates into actual resources reaching a part of Congo that is very hard to get to. The next few weeks will determine whether this becomes a contained regional outbreak or something much larger.
Also in the news… mifepristone, hantavirus, and COVID
May 15th
TFAH’s Ready or Not 2026 finds the U.S. faced compounding emergencies in 2025 (worst flu season in a decade, highest measles count since 1991, ongoing H5N1, major weather disasters) even as federal public health funding and workforce were destabilized. Across 10 preparedness indicators, 20 states ranked high, 17 plus DC middle, and 13 low, with strengths in nurse licensure portability and lab surge planning but gaps in funding stability, paid sick leave, flu vaccination, and hospital safety. TFAH calls for stable federal funding, restoration of 2025 workforce cuts, and reauthorization of the Pandemic and All-Hazards Preparedness Act.
May 13th