

The Harder You Push, the Harder They Push Back
From mask mandates to Ebola quarantines, the same psychology drives resistance to public health measures. Coercion triggers the opposite of compliance.


She tested negative. She had no symptoms. She refused the second test anyway.
What does this predict for the current Bundibugyo Ebola outbreak?
She tested negative. She had no symptoms. She refused the second test anyway.
She tested negative. She had no symptoms. She refused the second test anyway.
Angela Perryman tested negative for hantavirus. She had no symptoms. She had cooperated with the first round of blood tests at the National Quarantine Unit in Omaha, where she and 17 other Americans from the MV Hondius cruise ship were being held under a federal quarantine order.
Then she refused the second test.
Her explanation was simple: “At this point, I don’t actually trust them to use information responsibly. I’m no longer willing to offer them additional information because of a violation of trust.”
Three passengers from the same ship had already died. Andes hantavirus has a case fatality rate as high as 40%. The incubation period stretches to 50 days, meaning a negative test early on does not rule out infection. Further testing was clearly in her interest.
She refused anyway.
The psychology of doing the opposite of what you are told.
In 1966, psychologist Jack Brehm named a pattern he called psychological reactance. When people feel their freedom is being taken away, they push back, sometimes by doing the exact opposite of what they are told. The effect is strongest when the pressure feels forced, and the person never agreed to the rule.
Two things happen at once: anger at whoever is doing the pushing, and a hunt for reasons the rule is wrong. These are not steps. They feed each other. Psychologists call this the intertwined model. The person is not calmly weighing facts. They are building a case while feeling furious.
That is what happened with Perryman. She went along at first. But the quarantine kept going — held far from home, staff in hazmat suits, a federal order saying police could step in if she tried to leave. The pressure built. She went from giving blood to refusing tests to planning a lawsuit. The quarantine did not just fail to change her mind. It drove her the other way.
The same pattern scaled to millions during COVID.
Mask mandates were the clearest mass test of this pattern. A survey of more than 2,000 adults in the U.S. and Canada found that 16% refused to wear masks. Two factors drove the refusal more than any others: the belief that masks did not work, and a gut-level rejection of being forced.
The rule itself was the problem. People who might have worn a mask on their own pushed back when told they had to. Vaccination requirements reduced willingness to get the shot among people who were on the fence. Repeated messaging made it worse: the more people heard it, the more controlled they felt, and the less they followed the rules.
Money stress added fuel, but only when the rules were framed as a personal cost. When the same rules were framed as protecting the community, money stress stopped driving resistance. The framing changed the response.
In West Africa, the pattern ran deeper.
During the 2014-2016 Ebola epidemic, Liberia ordered the cremation of bodies and forced quarantine. Both set off fierce backlash. Cremation broke sacred funeral rites. Quarantine meant lost income, shame, and people fleeing. Wealthy families bribed burial teams for private burials while the poor had no choice. Communities shut out the official response and built their own.
In Guinea, we distinguished between réticence and résistance. Réticence meant reluctance, hesitation, something potentially negotiable. Résistance meant confrontation. The words shaped the response. Call it reluctance, and you send mediators. Call it resistance, and you send security. The framing mattered because everyday reluctance, hiding the sick, secret burials, delayed reporting, could harden into spectacular resistance, arson, riots, killings, when the lower-level frustration was not addressed.
In Sierra Leone, Ebola was widely denied until people witnessed it firsthand. Mass media health promotion was largely ineffective. What worked was testimony from survivors and directly affected community members, people the audience trusted, speaking from shared experience.
In Liberia, the pattern produced a single dramatic episode that reads like a textbook reactance case. In August 2014, residents of the West Point slum in Monrovia raided a holding center and patients fled. The government had imposed quarantine without food, water, or basic services. Residents described the quarantine as "aggression" and "an abuse of rights." When community-based teams later replaced the outside responders, they found more than 40 suspected cases and uncovered 34 secret burials that had gone unreported. Trust shifted when the messengers changed.
In North Kivu during the 2018-2019 DRC outbreak, things got worse. One in four people surveyed believed Ebola was made up. Trust in the government was very low. Armed guards escorted health teams. Patients ran.
This was not just reactance. It was reactance on top of decades of war, political neglect, colonial medical history, and poverty. Reactance explains how people pushed back: the anger, the counter-arguments, the concealment, the flight. But mistrust, structural violence, and political history explain why those measures were experienced as threats in the first place. A comparative study of Guinea and Sierra Leone found that the difference in resistance was better explained by political configurations and lived relations to authority than by cultural differences.
What does this predict for the current Bundibugyo Ebola outbreak?
The Ebola outbreak in eastern Congo and Uganda had the conditions for strong resistance from the start. What was easy to predict is now happening.
Bundibugyo ebolavirus kills fewer people — roughly 25-34% compared to 69-88% for Zaire ebolavirus. That sounds like good news. But it is making resistance worse. This strain does not look like the Ebola people expect. Patients show up with fever, stomach pain, and diarrhea — no bleeding in the early stages. It looks like malaria. Health workers missed it at first. Early tests came back negative because they were designed to detect Zaire ebolavirus, not Bundibugyo. People watched neighbors die while officials said there was nothing wrong. The Red Cross now believes three of its own volunteers contracted the virus on March 27 while handling bodies in Mongbwalu, a month before the first confirmed death. If true, the outbreak ran undetected for seven weeks. Trust broke before the response even started.
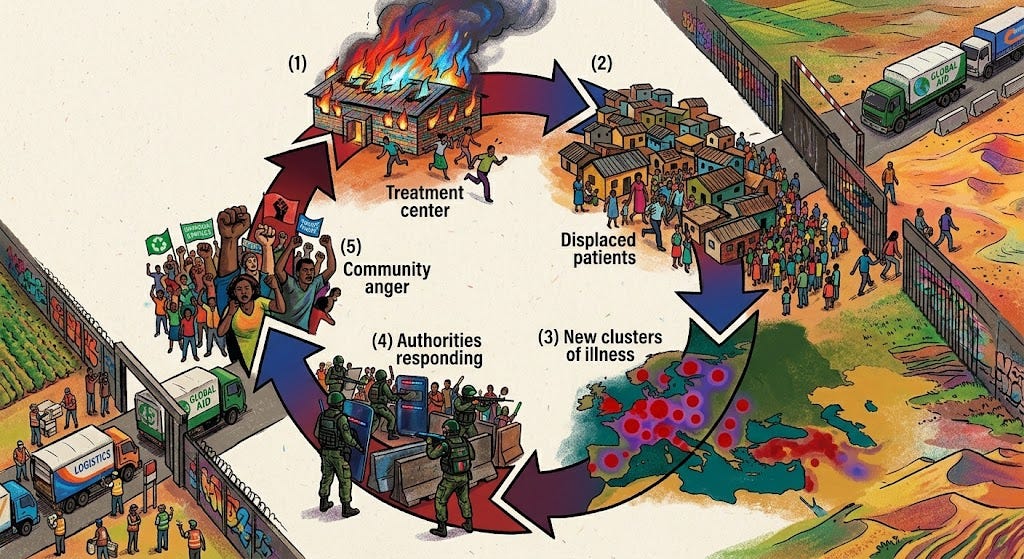
The resistance is no longer a prediction. On May 21st, a group of youths set fire to the Ebola treatment center at Rwampara Hospital after they were blocked from retrieving the body of a friend who had died. They accused the aid group running the center of lying about Ebola. Six patients were being treated. All survived, but six cases, three suspected and three confirmed, fled during the fire. Two days later, a second treatment tent was set on fire in Mongbwalu, this one run by Doctors Without Borders. Eighteen suspected Ebola patients escaped into the community. On Sunday, a third facility was attacked. Young men stormed Mongbwalu General Hospital as gunfire rang out, forcing staff to evacuate patients. Three attacks in one week, each bolder than the last. Patients who run become contacts nobody can trace. This is what happened in North Kivu in 2018 and 2019. MSF shut down.
The government's response has been enforcement. Ituri's provincial authorities banned funeral wakes and gatherings of more than 50 people. Burials can now only be conducted by specialized teams. Armed soldiers and police guard some burial sites. In Mongbwalu, a father lost his 16-year-old daughter to the disease and could not say goodbye. He was in isolation. She was buried by strangers. These are the same coercive measures that generated explosive backlash during the 2014 West Africa epidemic and the 2018 North Kivu outbreak.
The outbreak is also outrunning the response. The case count has roughly quadrupled in a week, from about 250 suspected cases to nearly a thousand, with more than 220 deaths. A confirmed case turned up in South Kivu, about 1,500 km from where the outbreak started. The area is held by the M23 armed group. The patient, 28, died before the test came back. Two contacts are already sick. The case was reported through rebel channels, not the national health system. Government response teams cannot work there.
The Title 42 order barring non-citizens from the DRC, Uganda, and South Sudan is pushing in the wrong direction. On May 22nd, the order was expanded to lawful permanent residents, green card holders, for the first time in the history of the statute. That same day, the WHO Emergency Committee explicitly recommended against flight suspensions and entry denials. Travel bans during the 2014 outbreak drove people to hide where they had been and to skip care. When Rwanda closed the Cyanika border crossing during the last outbreak, people moved to less-watched routes. The ban did not stop them. It made them harder to find. Rwanda’s current closure has also cut off the main route for aid into eastern Congo.
Only 36% of people surveyed trusted Ebola responders during the last outbreak. In Ituri Province, revivalist churches are holding multi-day prayer sessions for the sick. They are hiding patients and creating conditions for explosive spread. Local civil society leaders say the anger is driven largely by misinformation spread through churches and years of conflict. Some congregations have told their members the outbreak is fake. The DRC's own response plan now treats community resistance as the central challenge. It calls for talks with religious leaders, not enforcement.
What works is not force. It’s engagement.
The evidence across outbreaks points to the same set of tools.
Survivor messengers. In every Ebola outbreak studied, survivors have been the most trusted voices — more than mass media, outside experts, or government officials. When religious leaders in Sierra Leone spoke up for safe burial, the number of people willing to accept it nearly doubled. Sierra Leone's community engagement initiative eventually operated in all 14 districts through 2,466 community mobilizers, more than 6,000 religious leaders, and 42 radio stations. It was the largest coordinated community engagement effort of the entire West Africa epidemic.
Community framing. Telling people what they can do for their families works better than telling them what they must not do. In a randomized experiment, messages about what the community stood to lose beat every other approach.
Choice. Messages that named both the benefits and the limits of an action, and reminded people they were free to choose, cut resistance among the most hesitant.
Material support. People do not stay in quarantine without food, money, and basic services. The main reasons people break quarantine are lost income, not enough supplies, and shame, not stubbornness.
The pattern holds across every setting. One American refusing a blood test in Nebraska. Millions pushing back on mask rules. Treatment tents burning in eastern Congo. A father burying his daughter through strangers. Eighteen patients disappearing into the community.
Reactance is not a character flaw. It’s a normal psychological response to being pushed. Public health measures that ignore it do not just fail. They build the very resistance they are trying to break.
And in the news…
May 23rd
May 25th