The Ebola Disinformation Playbook Activated in Under 12 Hours
Within hours of the Bundibugyo PHEIC, the same conspiracy theories, supplement sales, and chain emails surfaced. Here’s the playbook and how to spot it.

The outbreak was hours old. The disinformation was already circulating.
The information outbreak runs on a faster clock than the disease.
The disinformation machine is funded. The counter-system is not.
The outbreak was hours old. The disinformation was already circulating.
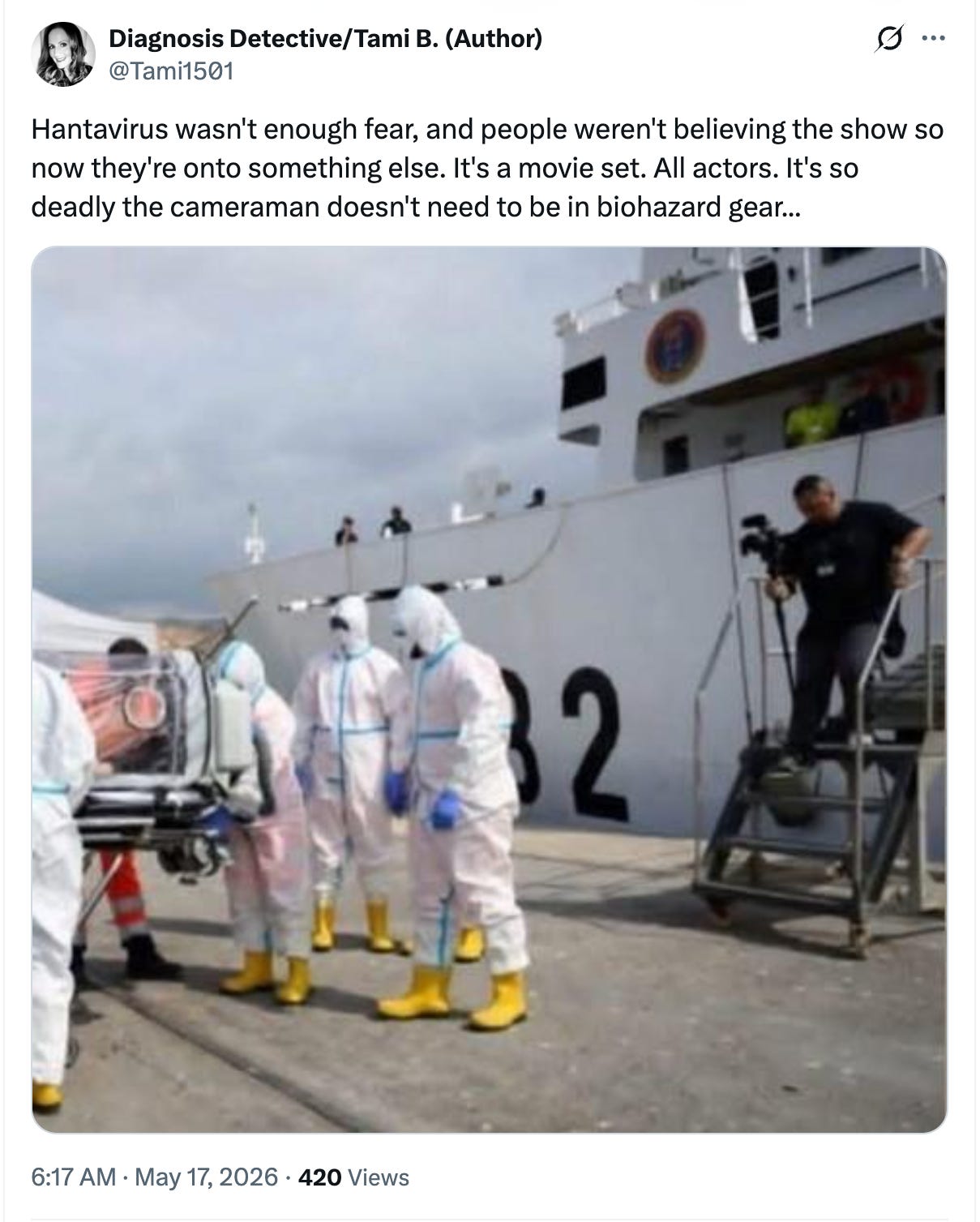
On the morning of May 17, 2026 — as the World Health Organization was declaring a Public Health Emergency of International Concern over a cross-border Ebola outbreak in the Democratic Republic of the Congo and Uganda — an account on X posted a photo of health workers in full biohazard gear boarding a ship. The caption declared the whole thing a movie set. All actors. The proof? A cameraman standing nearby without protective equipment.
The image wasn’t from the DRC. It wasn’t from Uganda. It appeared to be from the hantavirus cruise ship evacuation in Tenerife days earlier — a real public health operation, being used as evidence of a hoax. But that didn’t matter. The post was already doing what it was designed to do.
When I opened my email this morning, I had also received a chain message announcing that Ebola in the Congo could be stopped with baking soda dissolved in water. It also promised to cure Alzheimer’s.
The WHO’s emergency declaration cited eight confirmed cases, 246 suspected cases, and 80 suspected deaths from the rare Bundibugyo strain, a variant with no approved vaccine and no specific treatment. The virus had already crossed into Uganda, with two confirmed cases in Kampala, including one death. Case fatality rates in the two previous Bundibugyo outbreaks have ranged from 30% to 50%.
That is the outbreak. It is serious and deserves serious attention.
But what follows is what always follows. (keep scrolling past screenshots)
The information outbreak runs on a faster clock than the disease.
Within 48 hours of the first confirmed Ebola reports on May 15th, my social media monitoring account surfaced 640 Ebola-related videos across TikTok, Instagram, and YouTube — totaling over 68 million views. A separate search focused specifically on disinformation keywords — “ebola conspiracy,” “ebola bioweapon,” “ebola cure,” “ebola cover up” — returned 50 videos and 2.6 million views in the same period.
The accounts posting this content are not confused bystanders. Many of them are repeat players.
An account called @zelenko.labs, which sells a supplement called Z-Stack, posted a video asking, “What virus will they come up with next to scare you?” The solution: buy their zinc and vitamin D3 formula. The caption tagged #ebola, #norovirus, and #hantavirus, covering all bases. The same account had posted the day before about an alleged CIA cover-up of COVID’s origins. Z-Stack has never been tested in a clinical trial, and there is no evidence that it boosts immunity against any virus, let alone Ebola, which spreads through direct contact with infected bodily fluids and kills by attacking the immune system and blood vessels.
Another account, @dr.ashtoncaskey, posted a video noting how “interesting” it was that “all of these viruses are happening just before the World Cup.” The implication: the outbreak is manufactured fear, timed for maximum disruption. The video got over 9,000 views and a virality score of 20.73 — placing it among the top-performing Ebola content on TikTok that day.
On TikTok, @midnightwhispers673 asked: “lab accident or natural outbreak? the truth is terrifying.” Tagged: #conspiracy, #History, #coverup.
An astrology influencer with nearly 100,000 followers posted a video listing every major disease outbreak since 2014 — Ebola, Zika, COVID, monkeypox, bird flu, hantavirus — and attributed the pattern to Mars-Saturn conjunctions. The same post offered paid astrology readings.
Each of these accounts gains followers, views, and in some cases, direct revenue from the content. The supplement seller gets sales. The astrology influencer gets paying clients. The conspiracy account gets algorithmic amplification, which drives ad revenue and brand deals.
Someone is always selling something.
The 2025 Edelman Trust Barometer on health found that 21% of adults globally say content creators without medical training have influenced their health decisions. Among people aged 18 to 34, 45% say people without medical credentials have a big influence on their health choices. That same age group was the most likely to report regretting a health decision based on misinformation — 58% said they’d done so. The top source of that regret? User-created content on social platforms.
The National Academies of Sciences, Engineering, and Medicine released a landmark report in 2025 documenting the architecture. Some people spread misinformation with good intentions. They’re confused about what’s credible, or they’re not paying close attention to accuracy before they share. Others do it knowingly. The motives: profit financially, sell snake oils, accrue social rewards (followers, likes, shares), leverage their audience for advertising revenue and sponsorships, gain political power, erode trust in institutions, and/or create chaos.
A separate analysis of 53 top nutrition misinformation influencers found that 96% had a financial interest tied to the advice they shared — supplements, coaching, health consultancies, or paid events. The largest earned over $100,000 per month. The researchers sorted them into three categories: "Docs" who leverage or fabricate medical credentials, "Rebels" who build audiences by challenging mainstream guidance, and "Hustlers" who monetize fear through product sales. The categories apply well beyond nutrition.
Outbreaks are profitable content. Fear drives engagement. Engagement drives followers. Followers drive revenue.
The playbook doesn’t change. Only the virus does.
I’ve worked in (and also, since 2013, covered) infectious disease outbreaks since the late 1990s — HIV, tuberculosis, Ebola, Zika, MERS, chikungunya, COVID, mpox, hantavirus — am I missing any? Every new outbreak triggers the same disinformation playbook. The pathogen changes. The script does not.
Here is what you will see circulating over the coming days and weeks. Some of it is already here.
“It’s not real.” The outbreak is staged. The images are from movie sets. The health workers are crisis actors. The cameraman wasn’t wearing PPE, which proves it’s fake. (The cameraman wasn’t in direct contact with patients. Health workers were. That’s why they were in gear.) This is the claim in the @Tami1501 screenshot at the top of this piece.
“It’s a bioweapon.” Ebola was engineered in a lab — by the U.S. government, by China, by pharmaceutical companies, by the WHO itself. This theory circulated during the 2014 West African Ebola outbreak, when roughly 10% of Ebola-related tweets contained false or partially false information, and the most common conspiracy was that the outbreak was manufactured by political figures, media organizations, or pharmaceutical companies. It’s already circulating again. TikTok account @midnightwhispers673 asked “lab accident or natural outbreak?” within hours of the outbreak being confirmed.
“They’re doing this on purpose.” The timing is suspicious — right before an election, right before the World Cup, right before some other major event. The virus exists to distract you, to control you, or to justify government overreach. @dr.ashtoncaskey’s video linking the outbreak to the World Cup is this claim, repackaged.
“There’s a simple cure they don’t want you to know about.” Baking soda. Zinc supplements. Vitamin C. Elderberry. Alkaline water. Oregano oil. The forwarded email in my inbox is this claim. So is the @zelenko.labs video selling Z-Stack. These products are not treatments for Ebola. There are no approved treatments for the Bundibugyo strain. Supportive care — IV fluids, oxygen, blood pressure management — is what saves lives.
“The vaccine is the real danger.” Even though there is no approved vaccine for the Bundibugyo strain, expect claims that a future vaccine is the real threat. During the COVID pandemic, anti-vaccine conspiracy theorists seized on every sudden or unexplained death to blame vaccines — including the death of my late husband, journalist Grant Wahl, who died of a ruptured aortic aneurysm while covering the World Cup in Qatar. His autopsy was clear. The conspiracies never stopped. This pattern will repeat.
“Follow the money.” Pharmaceutical companies are orchestrating the outbreak to sell vaccines and treatments. The WHO declared a PHEIC to generate funding. Doctors are in on it. This framing exploits legitimate questions about pharmaceutical pricing and institutional accountability, then twists them into a blanket claim that the entire public health system is a fraud.
“It’s a pattern.” Every two years there’s a new virus — Ebola, Zika, COVID, monkeypox, bird flu, hantavirus, now Ebola again. This “proves” the outbreaks are planned. (Zoonotic spillovers are becoming more frequent. Humans are encroaching further into wildlife habitat. Global travel connects previously isolated populations. Climate change is shifting animal ranges. The pattern is real. The cause is ecological, not conspiratorial.)
How to recognize the playbook when you see it.
You don’t need a medical degree to spot outbreak disinformation. You need to know what to look for.
Check who benefits. Is the person posting selling something: a supplement, a course, a paid membership, a book? Are they asking you to follow, subscribe, or click a link in their bio? If the call to action is commercial, the content is marketing, not public health information.
Check the credentials. A TikTok account with 76 followers selling zinc supplements is not a public health authority. Neither is an astrologer, a “wellness coach,” or someone whose bio says “truth seeker.” The Edelman data shows your doctor is trusted by 82% of people for a reason. Content creators without medical training are trusted by far fewer people, but they’re louder online, and the platforms reward volume over accuracy.
Check the image. Disinformation often recycles old images from unrelated events. A reverse image search can tell you when and where a photo was actually taken. The biohazard-suit photo in the tweet at the top of this article is not from the current DRC outbreak.
Check the timing. If someone has a treatment protocol ready within hours of an outbreak announcement for a rare virus strain with no approved therapeutics, they did not develop that protocol in response to the outbreak. They are repurposing an existing sales pitch.
Check the emotional register. Disinformation tends to run hot — all caps, alarm emojis, “THEY DON’T WANT YOU TO KNOW,” “WAKE UP.” Reliable public health communication is specific, measured, and cites sources. It tells you what is known, what is not yet known, and what to do. It doesn’t yell.
Check whether they name the strain. This outbreak involves the Bundibugyo strain, which is clinically distinct from the Zaire strain that has driven most previous DRC outbreaks. If someone is telling you about “Ebola” without specifying the strain, they may not understand what they’re talking about, or they may not care, because the specifics don’t serve the narrative. Or maybe they just can’t spell or pronounce Bundibugyo.
The disinformation machine is funded. The counter-system is not.
The conditions that enable outbreak disinformation have worsened since COVID.
Trust in the media to report accurate health information has collapsed 13 points globally since 2019. The 2026 Edelman Trust Barometer found 70% of Americans now hold what researchers call an “insular mindset” — they’re hesitant or unwilling to trust anyone different from them. Among that group, journalists are trusted by just 31%.
The NAM report found that local journalism, the kind best positioned to provide community-specific, trusted health information, has been gutted. "News deserts" allow misinformation to fill the void. At the same time, USAID, which has been a central funder and coordinator of every major U.S. Ebola response, has had its funding cut. The CDC lacks a Senate-confirmed director. Social media platforms have scaled back content moderation.
The disinformation infrastructure, by contrast, is fully operational. It doesn’t need appropriations. It doesn’t need peer review. It doesn’t need to be accurate. It just needs an audience, and the platforms deliver one automatically.
Disinformation is a co-infection.
The WHO defines an “infodemic” as too much information, including false or misleading information, during a disease outbreak. The term makes it sound like an unfortunate byproduct, something that happens alongside the real emergency.
A more precise term: co-infection. Disinformation during outbreaks functions as an active pathogen in the information environment. It has vectors (social media platforms, email chains, group chats). It has superspreaders (high-follower accounts with financial incentives). It has a susceptible population (people who’ve lost trust in institutions, which is most of us). And it has real health consequences: people delay treatment, reject public health guidance, or take useless supplements instead of seeking care.
During the 2018-2020 Ebola outbreak in DRC, disinformation spread on Facebook and WhatsApp, blaming foreigners for the virus. That messaging contributed to armed attacks on Ebola treatment centers. Health workers were killed.
Disinformation gets people killed. That is documented history, not speculation.
The people who can help — epidemiologists, clinicians, community health workers, organizations like Médecins Sans Frontières who are on the ground right now — are working with real constraints and real risk. The people posting conspiracy theories from their apartments are not.
The next time someone forwards you an email promising a kitchen-counter cure for a hemorrhagic fever, delete it.
The baking soda will not help.