

Can Andes virus spread through the air?
Andes virus doesn’t spread like COVID, but saliva, breathing, and ventilation still matter.

High viral load, crowded events, and person-to-person spread
Andes virus has been found in human saliva and respiratory samples.
What we should do while scientists answer the remaining questions.
What we know and don’t know about Andes virus transmission.
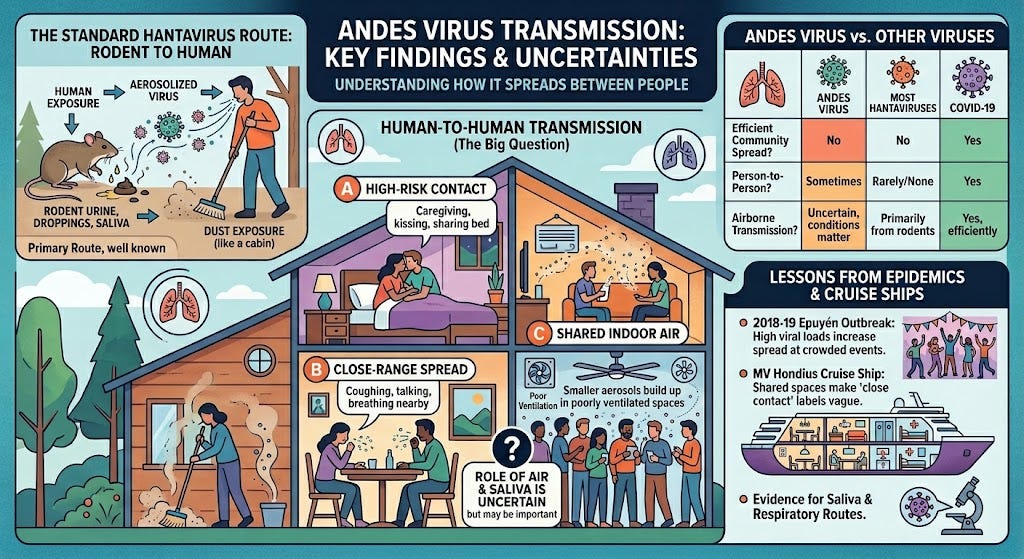
Andes virus can spread from one person to another. The harder question is how. Can it move through the air? Can someone get infected by sharing a room, cabin, dining area, or hospital space with a sick person? Or does it usually take closer contact: caregiving, kissing, sharing a bedroom, or being near someone for a long time?
The question matters because words like “close contact” can sound reassuring. They can make people think the air does not matter. We learned during COVID that this can be a mistake. On March 20, 2020, in an episode of my podcast Epidemic on “airborne versus droplet” spread, I spoke with science journalist Roxanne Khamsi and MIT researcher Lydia Bourouiba about why these labels can be too simplistic. Germs do not travel in neat boxes. This is also when I understood that COVID was airborne. (My dear friend Roxanne recently published Beyond Inheritance: Our Ever-Mutating Cells and a New Understanding of Health. It’s an excellent read. Here’s Dr. Jerome Groopman’s review of it in The New Yorker.) Some particles fall quickly. Others can stay in the air, build up indoors, and move with airflow.
Andes virus is not SARS-CoV-2, the virus that causes COVID. It does not seem to spread as easily through the air and has not shown the widespread community spread we saw with COVID, the flu, or measles. But Andes virus is also different from most other hantaviruses, which spread from rodents to people and then stop. Andes virus can sometimes keep spreading between people, especially in homes, crowded gatherings, caregiving situations, and poorly ventilated indoor spaces.
What we can say now: Andes virus spreads between people, and air and saliva may play a role. The risk appears highest in close, crowded, or poorly ventilated places. Scientists are still working out how often shared air is involved.
What “close and prolonged contact” leaves out.
Experts (including myself) have said that Andes virus spreads through “close and prolonged contact.”
That phrase is partly useful. It tells us the highest risk is usually among people who spend a lot of time near someone who is infected. That can include family members, sexual partners, caregivers, cabin-mates, or people at crowded events. But it does not tell us exactly how the virus moved.
People in the same home may share air, meals, bathrooms, bedrooms, towels, and caregiving duties. People on a cruise ship may share cabins, dining rooms, hallways, medical care, and ventilation. People at a wake or birthday party may speak face-to-face with a sick person, but they may also breathe the same indoor air for hours.
“Close contact” is probably too vague. It can make airborne spread sound impossible, even when the real answer is still uncertain. My friend Joseph Allen, a Harvard public health professor who studies indoor air quality, ventilation, and how buildings shape infectious-disease risk, recently raised this concern in an essay in The Atlantic: public health messages can become too reassuring before we fully understand how a virus spreads.
COVID taught a hard lesson about that. If shared air may matter, we should say so clearly.
High viral load, crowded events, and person-to-person spread
The best evidence for person-to-person spread comes from the 2018-2019 Epuyén outbreak in Argentina.
In that outbreak, one infection likely began with a rodent, and then the virus spread from person to person. Investigators found 34 confirmed infections and 11 deaths. Three sick people helped drive much of the spread after they attended crowded social events.
Before control measures were used, each infected person caused about 2.12 new infections on average. After isolation, quarantine, and contact tracing began, that number fell to 0.96 — indicating the outbreak slowed as people were separated and their contacts were monitored closely.
The study also found that people with high viral loads were more likely to spread the virus. (Viral load means how much virus is in a person’s body.) People with signs of liver injury were also more likely to spread it. Age, how sick a person looked, time in the hospital, and small genetic changes in the virus did not clearly explain who spread it.
People carrying a lot of virus, who also had many chances to expose others, were the likeliest to pass Andes virus on.
Three ways a virus can spread through the air
When we ask whether Andes virus spreads through the air, we need to be clear about what that means, because there are at least three possibilities.
The first is the usual hantavirus route. People breathe in virus from rodent urine, droppings, or saliva. This can happen when someone cleans, sweeps, or disturbs a space with infected rodents. This route is well known. CDC guidance says people mostly get hantavirus by breathing in virus from infected rodents’ body fluids and waste.
The second is close-range spread from a sick person. A person may breathe, talk, cough, or share saliva at close range, releasing virus-containing particles near another person.
The third is shared indoor air. Smaller particles may stay in the air longer, especially in closed or poorly ventilated rooms. These particles may build up over time in cabins, dining rooms, hospital rooms, or other crowded indoor spaces.
For Andes virus, the third possibility is the biggest open question. We do not have proof that it spreads widely through shared air the way COVID can. The International Hantavirus Society says there is no evidence that Andes virus spreads efficiently in the community like highly contagious respiratory viruses. But that does not mean air never matters. It means Andes virus has not shown COVID-like spread.
Air may matter most when people are close together, indoors, and sharing poorly ventilated spaces for a long time — conditions that can exist on a cruise ship such as the MV Hondius, where repeated exposure in cabins, dining rooms, hallways, and spaces used to provide medical attention can make it difficult to separate close contact from shared-air risk.
Andes virus has been found in human saliva and respiratory samples.
Scientists have reason to study saliva and respiratory spread in Andes virus.
A major review in The Lancet Infectious Diseases says Andes virus is unique among hantaviruses because it can spread from person to person. It also points to evidence that respiratory and salivary routes may be involved.
The International Hantavirus Society says Andes virus genetic material has been found in several kinds of patient samples, and infectious virus has been recovered from patient-derived materials. That supports the idea that human-to-human spread is biologically possible, but it does not yet tell us which route matters most — saliva, larger droplets, smaller aerosols, contaminated secretions, or direct contact.
We should take respiratory spread seriously, even though Andes virus does not seem to spread through the air as easily as SARS-CoV-2.
What makes a virus more or less transmissible.
Whether a virus spreads well depends on several things working together.
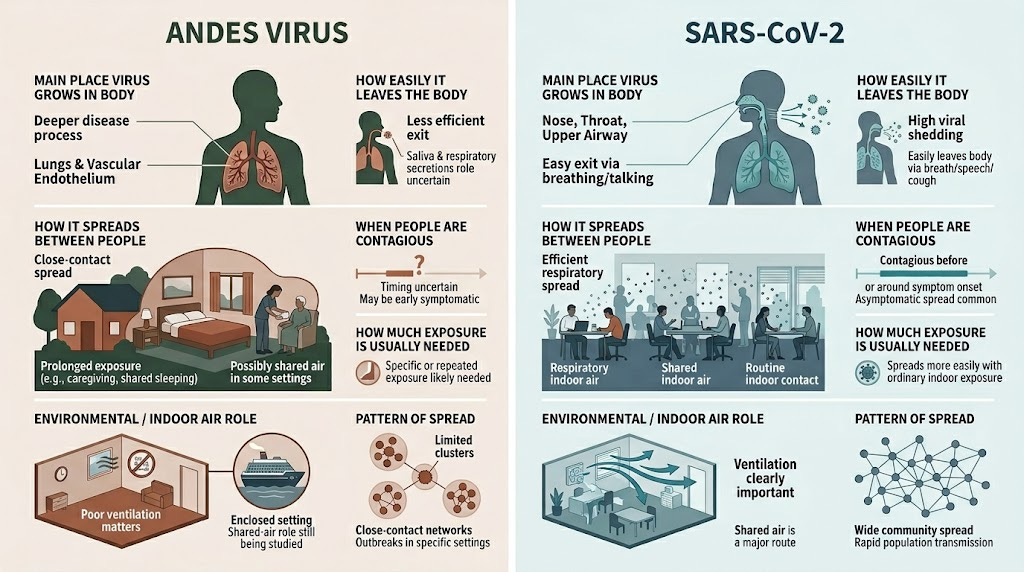
It has to leave the body easily. SARS-CoV-2 grows well in the nose and throat, so it gets out through breathing, talking, coughing, and singing. For Andes virus, this is less clear. The virus has been found in saliva and respiratory samples, but we still do not know how much infectious virus people actually release into the air.
It also has to survive long enough outside the body to reach someone else. Andes virus is an enveloped virus, and enveloped viruses tend to be more fragile outside the body than non-enveloped ones. That does not mean it cannot spread, especially indoors at close range, but it may limit how far and how long the virus can travel.
Entry point matters, too. SARS-CoV-2 infects cells in the upper airway, which is why the nose and throat work as both entry points and exit points. Andes virus causes severe disease partly by infecting the cells that line blood vessels, especially in the lungs. That may make it dangerous once infection takes hold, but less efficient at jumping from one person to the next.
Then there is infectious dose, meaning how much virus it takes to start an infection. For Andes virus, we do not yet know the infectious dose for human-to-human spread. If it is high, that would help explain why close, repeated, or prolonged exposure seems to matter more than brief contact.
Timing plays a role as well. SARS-CoV-2 can spread before symptoms appear, which made it very hard to contain. For Andes virus, scientists are still studying when people become contagious. If most spread happens after symptoms begin, isolation works well. If some spread happens earlier, contact tracing and monitoring become more important.
Finally, the setting matters. Even a virus that does not spread easily can cause a cluster when people are together indoors for a long time with poor ventilation. That is part of why the MV Hondius outbreak raised so many questions. A cruise ship turns many small risks into repeated exposures.
Andes virus is not the next COVID. But some risks overlap.
SARS-CoV-2 is very good at spreading through the air. It grows well in the nose and throat. People can spread it before they know they are sick. It can move through normal indoor activities: talking, breathing, singing, coughing, eating together, and spending time in rooms with poor ventilation.
Andes virus appears to spread less easily and seems to need more specific conditions: close contact, high viral load, crowded settings, caregiving, shared sleeping space, or indoor spaces where people spend extended time together. Scientists are still studying exactly when a person with Andes virus becomes contagious, and some experts warn that we should not assume people can spread it only after they are obviously sick.
So Andes virus is not the next COVID. But it can still use some of the same opportunities: indoor air, close contact, crowding, and delayed recognition. That is why ventilation, masks or respirators in high-risk care settings, isolation, and contact tracing may all matter during an outbreak. This is why clinicians and public health workers interacting with known hantavirus patients and high-risk contacts should wear personal protective equipment.
When everyone on a ship counts as a close contact
The MV Hondius cruise ship outbreak made people pay closer attention to the air question.
A cruise ship is a hard place to control infection. People share cabins, dining rooms, hallways, medical spaces, excursions, and indoor air. They are together for days or weeks. If someone gets sick, it can be hard to separate people quickly.
Reports from the ship described several suspected or confirmed hantavirus cases and deaths. The World Health Organization confirmed that the virus was Andes virus. In The Atlantic, Kat Wu described how the outbreak unfolded in a closed setting.
Different countries have chosen different quarantine plans because the science is still uncertain.
The cruise outbreak does not prove that Andes virus spreads easily through the air. But it shows why “close contact” may not be enough to explain risk in closed spaces. On a ship, many people may count as close contacts. The harder question is which exposures mattered most: sharing a cabin, caring for a sick person, eating together, standing near someone, or sharing indoor air over time.
Don’t say it’s COVID. Don’t say air doesn’t matter.
Public health messages should avoid two mistakes.
The first is saying Andes virus spreads like COVID. The evidence does not show that. The second is saying only very close contact matters. The evidence is still too uncertain for that.
A clearer message would be: Andes virus usually spreads from infected rodents to people. It can also spread between people. Scientists are still studying the exact route. Saliva and respiratory particles may play a role. Risk appears highest with close, repeated, or prolonged exposure, especially in homes, caregiving, intimate contact, crowded gatherings, and poorly ventilated indoor spaces.
That message points toward practical steps. Sick people should be isolated. Caregivers and health workers should use proper protective equipment. Indoor air should be improved when possible through ventilation and filtration. Crowded indoor gatherings should be reduced during an investigation. Exposed people should be monitored because symptoms may take weeks to appear — one study estimated the incubation period for Andes virus could range from 7 to 39 days, with a median of 18 days.
What we should do while scientists answer the remaining questions.
Andes virus is not COVID, but it is also not a typical hantavirus. Most hantaviruses spread from rodents to people and stop there. Andes virus can sometimes spread from person to person, and the disease can be severe. The exact role of air is still being studied. Respiratory particles and saliva may matter, especially in close, crowded, or poorly ventilated places.
The lesson from my March 2020 Epidemic episode on airborne versus droplet spread still applies: we should not let simple labels get ahead of the science.
For Andes virus, the best message is measured caution. Do not treat it like COVID. Do not dismiss shared air. Protect people in high-risk settings while scientists answer the remaining questions: when patients become contagious, how much virus they shed in saliva and breath, whether infectious virus is present in aerosols, how ventilation affects risk, and which contacts truly need quarantine.