

Teaching Doctors About Nutrition Won’t Fix America’s Food System
Doctors need more nutrition training, but the food environment is the bigger driver chronic disease.

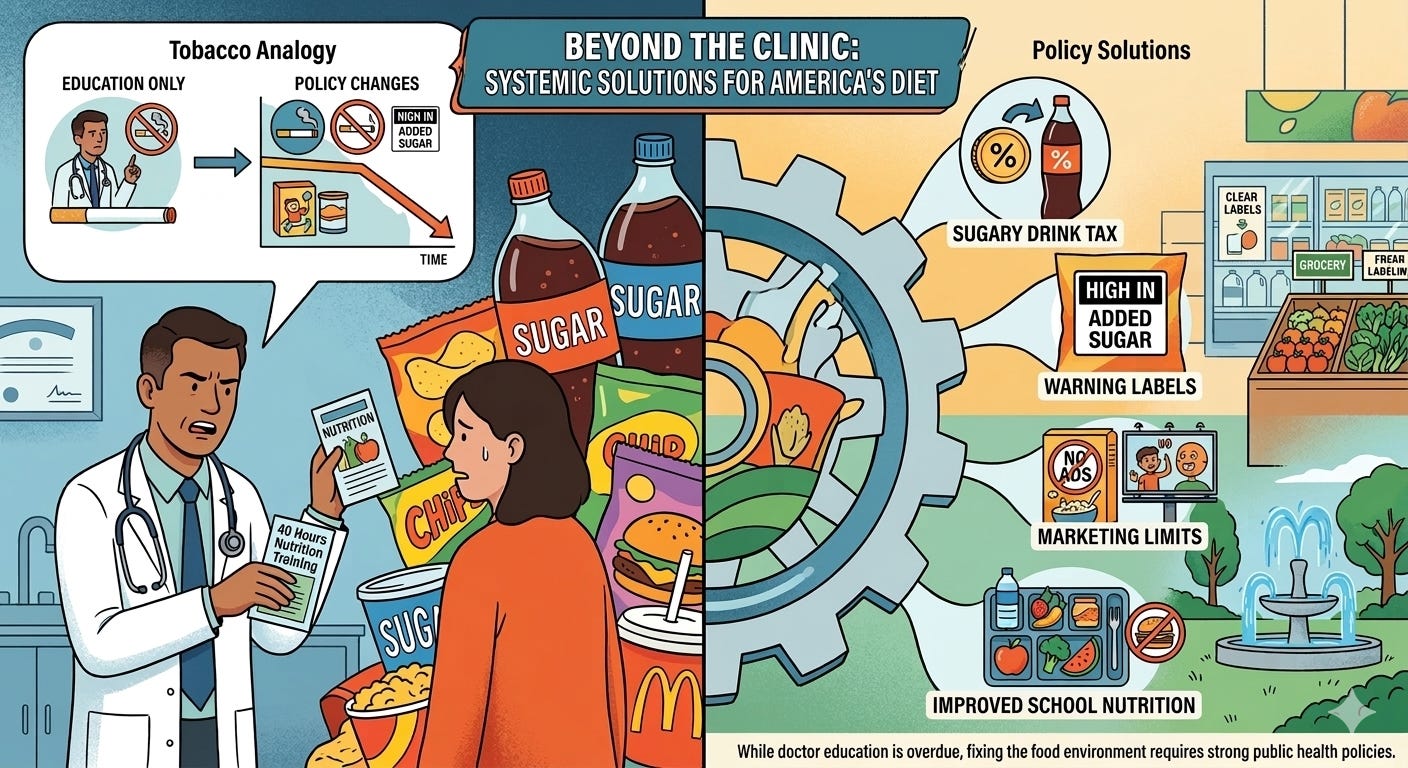
The limits of fixing diet through medical education
On Thursday in Washington, federal health officials announced a push to teach doctors more about nutrition.
“Today we mark an historic announcement,” Health and Human Services Secretary Robert F. Kennedy Jr. said. “Fifty-three medical schools across 31 states… will require every medical student to complete 40 hours of nutrition training.”
The move targets a long-recognized gap: many physicians receive little formal training in nutrition despite treating diet-related disease every day.
More training is overdue. But doctors alone cannot fix America’s diet. The real driver of chronic disease is the food environment itself, dominated by ultra-processed foods and added sugar.
Medical schools already face hard choices
Medical schools have finite time and an expanding list of subjects.
Students must master genetics, pharmacology, infectious diseases, surgery, and communication with patients. New topics, like artificial intelligence, are also competing for space.
Every new topic pushes another aside.
Nutrition is one clear gap. Many physicians receive fewer than 20 hours of nutrition education in medical school, and surveys show many feel unprepared to counsel patients about diet, obesity, and metabolic disease.
Doctors consistently report needing more training in practical skills like dietary counseling and obesity management. Medical training has traditionally emphasized diagnosing disease more than preventing it.
Surveys of medical students and doctors also show gaps in training on physical activity counseling, sleep, stress, and behavior change — all central to chronic disease prevention.
Ironically, medical students often struggle with healthy habits themselves. Long hours and stress mean poor sleep, little exercise, and irregular diets.
Other under-taught areas include mental health, addiction, women’s health, social determinants of health, health policy, and communication skills.
Doctors do not have to carry all expertise alone. Dietitians and other clinicians also play critical roles in helping patients improve their diets. They often have more time to spend with patients and can provide this care more effectively and at lower cost.
Lessons from tobacco control
Public health experience shows that education alone rarely shifts population health.
Smoking offers the clearest example.
Doctors advising patients to quit helped. So did nicotine patches and counseling.
But the biggest declines in smoking happened after major policy changes:
These policies changed the environment around smoking.
Ultra-processed foods dominate the American diet
More than half of the calories Americans consume come from ultra-processed foods, and the proportion is even higher for children.
These industrial products combine refined starches, added sugar, unhealthy fats, salt, and additives.
They are engineered to taste good, last on shelves, and be eaten quickly.
They are heavily marketed and everywhere.
Sugary drinks: a major source of added sugar
Sugar-sweetened beverages are one of the largest sources of added sugar in the American diet.
These drinks include:
soda
sports drinks
energy drinks
sweetened teas
other flavored beverages
Liquid calories behave differently than solid food. They don’t create the same feeling of fullness. As a result, people often drink these calories in addition to their meals.
Research has linked sugary drinks to a higher risk of:
obesity
type 2 diabetes
heart disease
fatty liver disease
The American Heart Association recommends limiting added sugar to 25 grams per day for women and 36 grams per day for men.
A single sugary beverage may contain most, or even more than, a full day’s recommended limit in one serving.
Because they are widely consumed and easy to measure, sugary drinks are a major focus of public health policy.
Policies that change behavior
Researchers have studied several ways to reduce sugary drink consumption.
The strongest evidence comes from taxes on sugary drinks.
Several U.S. cities — including Philadelphia, Seattle, San Francisco, Oakland, and Boulder — have implemented these taxes.
After the taxes were introduced:
prices rose about 33%
purchases of sugary drinks fell by about one-third
Researchers also found consumers did not appear to travel to nearby cities to avoid the tax.
Other policies, such as improving beverage standards in schools or making water the default drink in kids’ meals, can also help shift habits.
Doctors need training, but the food system needs reform
Improving nutrition education in medical school necessary.
Doctors should understand how diet affects chronic disease and feel comfortable discussing nutrition with patients.
But doctors alone cannot overcome a food system where ultra-processed foods dominate grocery shelves and sugary drinks remain cheap, heavily marketed, and easy to buy.
Solving America’s chronic disease crisis will likely require broader changes, including:
reducing added sugar in foods and drinks
limiting marketing to children
improving school nutrition standards
using pricing policies that discourage sugary drinks
Doctors need better nutrition training. But fixing America’s diet will require changing the food system itself.
Isn't it a thought process that there exists registered Nutritionists, would be the appropriate source, for reference, concerning nutrition, in the same manner that doctors would reference a patient to a qualified specialist in certain discipline?