

Why Fewer Pregnant Women Are Starting Care in the First Trimester
New federal data show declines between 2021 and 2024, with wide variation by race, insurance coverage, and location.

Early prenatal care declines nationwide
For nearly a decade, early prenatal care in the United States had been inching upward. More pregnant women were seeing a clinician in the first three months of pregnancy, a critical window for confirming due dates, screening for health conditions, and identifying risks that can affect both mother and baby. Now that progress has stalled and begun to reverse.
New federal data released today by the National Center for Health Statistics show that first-trimester prenatal care declined between 2021 and 2024. In 2021, 78% of mothers began care in the first trimester. By 2024, that figure had fallen to 76%. During the same period, second-trimester starts rose from 15% to 17%, and late or no care increased from 6% to 7%.
The COVID pandemic disrupted health care systems nationwide. The new figures suggest that early prenatal care has not returned to its pre-pandemic trajectory.
Differences across groups and states
National averages do not tell the whole story.
From 2018 to 2022, 78% of U.S. births involved first-trimester prenatal care, but there were significant differences by race and ethnicity. White mothers had early care rates above 82%, while Native Hawaiian and Other Pacific Islander mothers had rates near 60%. Late or no prenatal care exceeded 10% among Black and Hispanic mothers. Foreign-born mothers were also less likely to begin care in the first trimester compared with U.S.-born mothers.
Among teenagers, first-trimester care fell from 62% in 2021 to 57% in 2024, while late or no care rose from 13% to 15%.
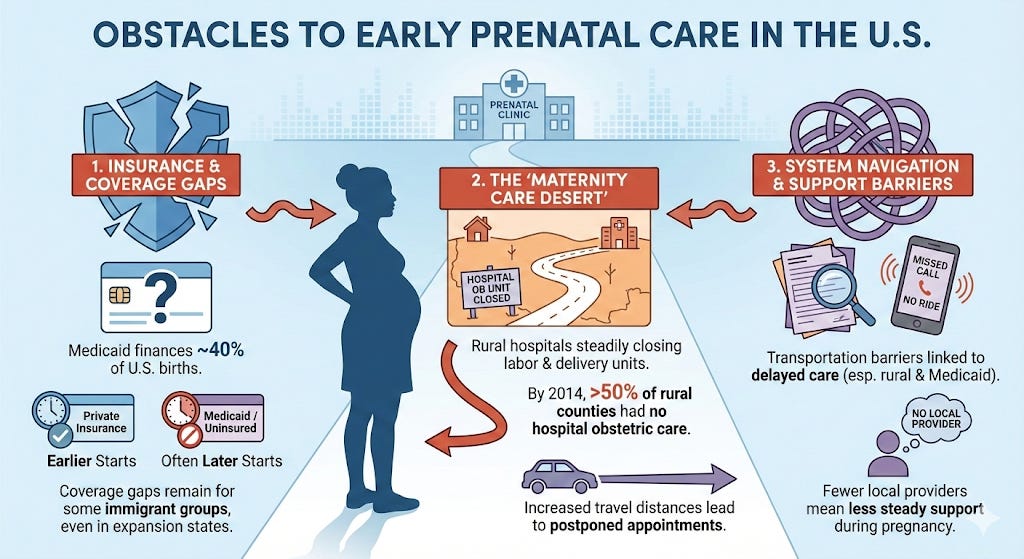
Insurance coverage is another factor. Medicaid finances about 40% of births in the United States, and women with Medicaid coverage are more likely to begin prenatal care later than women with private insurance.
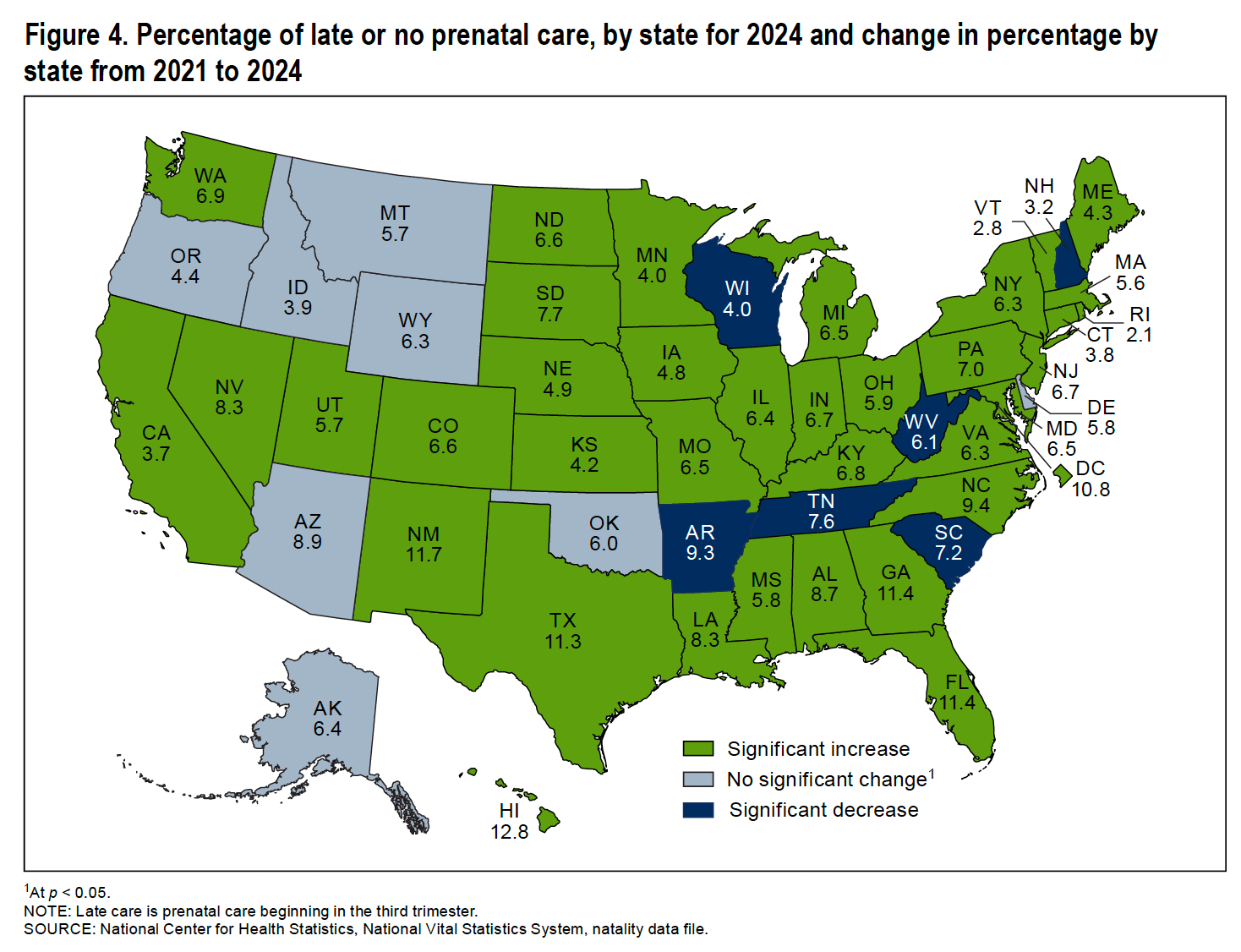
First-trimester prenatal care rates vary widely across states, and geographic differences have also grown. More than 2 million women of childbearing age live in counties without hospital-based obstetric services, often called “maternity care deserts,” and rates of timely prenatal care are lower in those areas.
Between 2021 and 2024, late or no prenatal care increased in more than three dozen states and the District of Columbia. In several states, more than one in ten mothers received late or no care in 2024.
Medicaid expansion and coverage gaps
Over the past decade, many states expanded Medicaid under the Affordable Care Act. As of 2026, most states have adopted expansion, though some have not.
Researchers have studied whether expansion affected prenatal care.
A 2021 study found that Medicaid eligibility reduced the number of women who were uninsured before pregnancy and slightly increased the share who received adequate prenatal care overall.
Another study in 2022 looked at immigrant and U.S.-born women in Medicaid expansion states. Before expansion, about 76% of immigrant women and 80% of U.S.-born women began care in the first trimester. After expansion, early prenatal care increased among U.S.-born women but did not increase in the same way among some immigrant groups. Eligibility limits tied to immigration status may have affected who benefited from the policy.
But insurance coverage is only part of the story.
When the hospital is far away
Even with insurance, care must be available nearby.
In many rural communities, the closest place to give birth is getting farther away. Over the past two decades, rural hospitals have steadily closed their labor and delivery units.
Between 2004 and 2014, 9% of rural counties lost hospital-based obstetric services. By 2014, more than half of rural counties had no hospital offering obstetric care.
When a local obstetric unit closes, pregnant women often must travel to another county for care. Counties losing services are more likely to be lower-income and have higher shares of Black residents.
When rural counties lose hospital-based obstetric services, women are more likely to give birth in out-of-hospital settings or in hospitals without obstetric units. Rates of preterm birth are also higher in counties that have lost obstetric services compared with counties that have kept them.
When a hospital closes its labor and delivery unit, the effects can ripple beyond the delivery room. Pregnant women may need to travel farther not only to give birth, but also for prenatal checkups. In some communities, fewer local providers mean fewer chances to build steady support during pregnancy.
Multiple studies have found that transportation barriers are linked to delayed prenatal care, particularly in rural communities and among Medicaid enrollees, who report higher rates of missed or postponed appointments.
As access to hospital-based maternity care changes, some states are exploring other ways to strengthen support for pregnant women.
Could doulas and community health workers help?
As some communities lose local maternity services, states are also looking at ways to strengthen support during pregnancy.
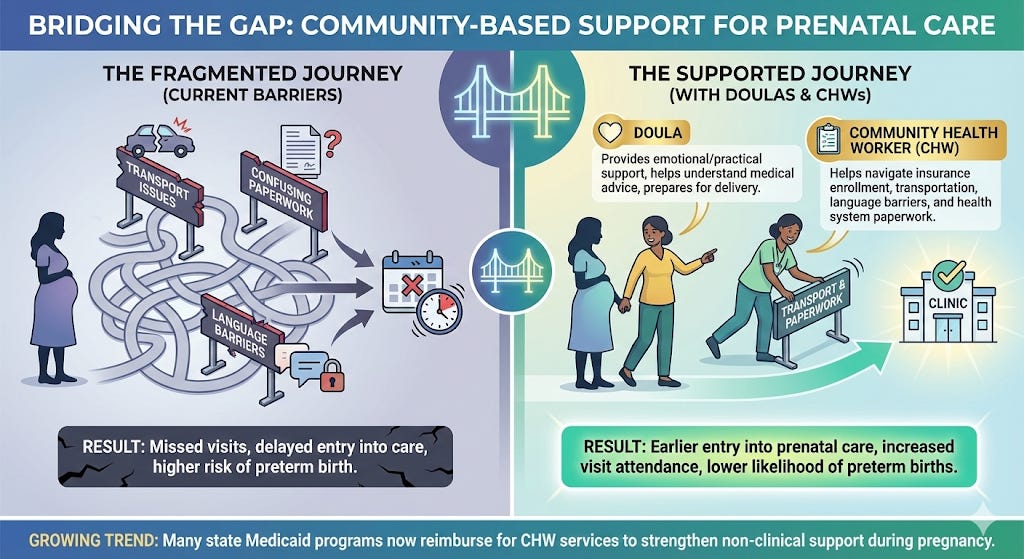
One approach is expanding access to doulas. Doulas are trained professionals who provide emotional, informational, and practical support during pregnancy and childbirth. They do not provide medical care, but they often help women schedule appointments, understand medical advice, and prepare for delivery.
Researchers studying a community-based doula program serving low-income women found that women who received doula support were more likely to attend prenatal visits and less likely to have preterm births than similar women who did not receive doula care. Doulas may help women stay connected to care by assisting with appointment scheduling, transportation planning, and navigating the health system.
Another approach involves community health workers (CHWs). Like doulas, CHWs often work in the community and help patients overcome barriers to care. A large review by the Agency for Healthcare Research and Quality found that CHW programs were associated with earlier entry into prenatal care and increased prenatal visit attendance, especially among low-income and minority women. CHWs are particularly effective in helping women navigate insurance enrollment, transportation, language barriers, and health system paperwork.
In recent years, more states have begun using Medicaid to support both doulas and community health workers. According to KFF, many state Medicaid programs now reimburse CHW services, including health education, outreach, care coordination, and help navigating the health system. States vary in how they certify providers and structure payments, but the overall trend reflects growing interest in strengthening non-clinical support during pregnancy.
Access, coverage, and what happens next
The new federal data do not point to a single cause for the decline in early prenatal care. Instead, they suggest that timing depends on several factors at once: insurance coverage, provider availability, transportation access, and support navigating the health system.
Whether first-trimester care rebounds may depend on how those pieces fit together. As states adjust Medicaid policies, respond to hospital closures, and expand community-based support, researchers will be watching to see whether early prenatal care returns to its previous trajectory, or whether the recent decline reflects a broader shift in access to maternity care across the country.