

CDC Used Title 42 to Ban Travelers Over Ebola. Its Own Order Explains Why That Won’t Work.
Title 42 sat unused for decades, then became an immigration tool during COVID. Now the CDC has invoked it for Ebola, a disease the order itself says can’t be transmitted by asymptomatic cases.

CDC issued a travel ban. The order explains why it won’t work.
Thomas Eric Duncan wasn’t stopped by a travel ban. He was failed by an ER.
If the risk is asymptomatic travelers, the exemption defeats the purpose.
How Ebola became a 2014 campaign issue and then vanished from the headlines.
Containing Ebola at the source costs less than banning travelers at the border.
CDC issued a travel ban. The order explains why it won’t work.
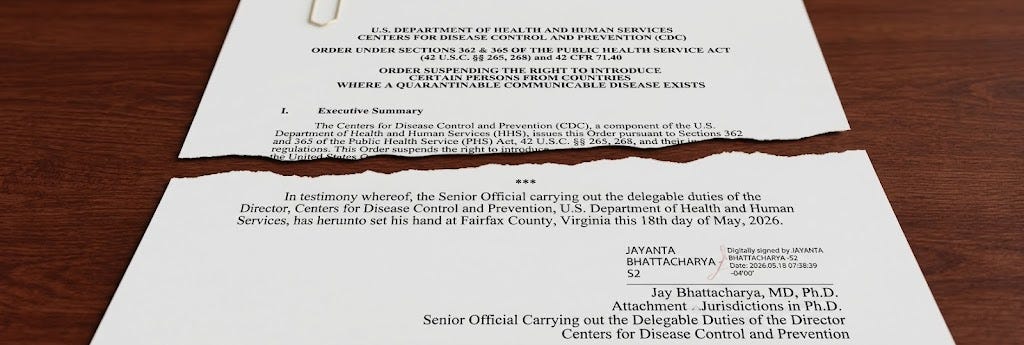
On May 18th, the Centers for Disease Control and Prevention issued a Title 42 order suspending the entry of non-citizens who have been in the Democratic Republic of the Congo, Uganda, or South Sudan in the past 21 days. The order cites an ongoing outbreak of Ebola disease caused by the Bundibugyo virus. It is signed by Dr. Jay Bhattacharya, identified as “Senior Official Carrying out the Delegable Duties of the Director.” Dr. Bhattacharya’s legal term as Acting CDC Director has expired (the Federal Vacancies Reform Act limits how long someone can serve as "acting" without a Senate-confirmed nomination).
The order describes the disease precisely. It also describes, in considerable detail, why the policy it enacts does not match the disease it cites.
Thomas Eric Duncan wasn’t stopped by a travel ban. He was failed by an ER.
Bundibugyo virus spreads through direct contact with the bodily fluids of a symptomatic person. It does not spread through the air, through respiratory droplets, or by sitting next to someone on a flight from Entebbe to Dulles. The order itself states that “infected individuals do not spread the virus until symptoms begin.”
This matters because the justification for the ban rests on a different scenario: an asymptomatic traveler who has been exposed to Ebola boards a plane, arrives in the United States, and later becomes sick. That is a real possibility. It happened in 2014, when Thomas Eric Duncan flew from Monrovia to Dallas while asymptomatic and later developed Ebola. He died. Two nurses who treated him at Texas Health Presbyterian were infected.
Duncan arrived in Dallas on September 20, 2014. He developed symptoms on September 24. He went to the Texas Health Presbyterian emergency room late on the night of September 25, told the nurse he had just arrived from Liberia, and was sent home with antibiotics. He returned by ambulance on September 28. What failed wasn’t the border. It was a hospital that didn’t isolate a patient with a fever who told them where he’d been.
If the risk is asymptomatic travelers, the exemption defeats the purpose.
The public health evidence on travel bans for infectious disease is extensive and largely unfavorable. Bans can delay the first imported case by days or weeks. They do not prevent outbreaks. For Ebola specifically — a disease that requires contact with bodily fluids and is not contagious until symptoms appear — the established countermeasures are exit screening in affected countries, entry screening and monitoring at arrival, 21-day follow-up of contacts, and hospital preparedness for isolation and treatment. (I underwent exit screening, entry screening, and 21-day follow-up when I traveled back from Guinea in 2015; so did my friend Dr. Craig Spencer, who was hospitalized for Ebola at Bellevue Hospital following his return. He did not infect anyone else.)
These are the tools the United States used during the 2014 West Africa Ebola outbreak, which infected more than 28,000 people across three countries. No travel ban was imposed. The CDC, the WHO, and the Obama administration all explicitly opposed one.
The same approach was used during the 2018-2020 Kivu Ebola outbreak in eastern DRC — 3,470 cases, the world’s second-largest Ebola outbreak on record. Again, no travel ban. The response relied on contact tracing, vaccination of contacts with the rVSV-ZEBOV-GP vaccine, and coordination with affected countries.
In declaring this Ebola outbreak a Public Health Emergency of International Concern, WHO recommended exit screening, contact monitoring, and testing, and explicitly recommended against any ban on international travel or trade.
The CDC Title 42 order was issued the next day.
Why travel bans make Ebola harder to contain.
Travel bans for Ebola don’t just fail to prevent importation. They can also undermine the response.
Countries that face economic penalties for reporting outbreaks — lost trade, lost tourism, suspended travel — have less incentive to report transparently. The International Health Regulations exist in part because of this dynamic: the global system depends on affected countries sharing surveillance data quickly, and it falls apart when those countries are punished for doing so.
Travel bans also disrupt the movement of health workers and supplies into affected areas. Containing Ebola requires trained responders on the ground — epidemiologists, lab technicians, infection prevention specialists, logistics staff.
And bans push travelers into indirect routes that are harder to track. A person who might have flown directly from Nairobi to JFK, and been screened on both ends, instead routes through three or four countries. The screening systems that work for direct travel break down when itineraries become opaque.
Travel bans are politically popular. During the 2014 outbreak, 67% of Americans supported one. But, for a disease like Ebola, what matters more is what happens after a traveler arrives: whether the hospital screens for travel history, whether the patient is isolated, whether contacts are traced. A travel ban is, however, more visible to Americans than work on-the-ground, in-country.
U.S. citizens carry the same risk. But they’re exempt.
If the risk is asymptomatic travelers, the exemption defeats the purpose.
The Title 42 order applies only to non-citizens. U.S. citizens and lawful permanent residents who have been in DRC, Uganda, or South Sudan are exempt. The order states that restricting non-citizen entry would allow public health authorities to “concentrate finite surveillance, screening, contact tracing, quarantine management, and medical monitoring resources on returning U.S. citizens and lawful permanent residents.”
The Bundibugyo virus does not distinguish between citizens and non-citizens. A returning American aid worker exposed to Ebola in Ituri Province carries the same risk as a Congolese business traveler. If anything, the order’s own logic — that the 21-day incubation period allows infected travelers to arrive before symptoms appear — applies equally to both groups.
The Duncan case, again, is instructive. He was a Liberian national. But the two people who contracted Ebola from him were American citizens — healthcare workers in a Dallas hospital.
From quarantine law to immigration tool.
Title 42 is a provision of the Public Health Service Act, enacted in 1944 and based on federal quarantine authority dating to 1893. It lets the CDC director block people from entering the United States when a dangerous infectious disease is spreading in another country. Before COVID, it had almost never been used.
That changed in March 2020, when the Trump administration invoked Title 42 to expel migrants at the southern border, citing COVID, a disease that can be transmitted by asymptomatic persons. Between March 2020 and May 2023, the United States carried out nearly 3 million Title 42 expulsions.
CDC officials at the time questioned the scientific basis for using the authority that way. Courts intervened. The Biden administration attempted to end it, then extended it, and it finally expired in May 2023.
A disease-based ban on top of an immigration ban.
South Sudan has been under a full U.S. travel ban since December 2025, one of seven countries added to the expanded ban list. The stated reasons were visa overstay rates and the South Sudanese government’s refusal to accept its own nationals being deported from the United States. The State Department revoked all South Sudanese visas in early 2025.
DRC and Uganda were among 36 countries — mostly in Africa — given a deadline in June 2025 to strengthen vetting procedures or face further restrictions. In January 2026, the State Department paused all immigrant visa issuances for nationals of both countries, citing high rates of public benefits usage. Tourist and other non-immigrant visas remained available until now. The Title 42 order closes that remaining avenue.
South Sudan went from visa revocation to full travel ban to Ebola-based entry suspension — three rounds of restrictions, each with a different stated justification, none related to the others. DRC and Uganda went from the 36-country watchlist to an immigrant visa freeze to a Title 42 suspension.
How Ebola became a 2014 campaign issue and then vanished from the headlines.
This is not the first time an Ebola outbreak has led to travel ban demands. During the 2014 West Africa epidemic, Donald Trump — then a private citizen — tweeted about Ebola nearly 100 times in three months, calling for a travel ban and demanding that President Obama resign. Seventy-four members of Congress, including nine Democrats, called for restrictions. Two Democratic Senate candidates in competitive races — Kay Hagan in North Carolina and Michelle Nunn in Georgia — broke with the Obama administration to support a ban.
Ebola became the October surprise of the 2014 midterms. In the four weeks before the election, the major broadcast and cable networks ran nearly 1,000 evening news segments on Ebola. CNN alone aired 335 segments. Fox News aired 281.
In the two weeks after the election, CNN’s coverage dropped to 10 segments. Fox dropped to 10. The last American Ebola patient was discharged from the hospital. The issue disappeared.
No travel ban was ever imposed.
The man who opposed lockdowns just signed a travel ban.
The Title 42 order is signed by Dr. Bhattacharya, who co-authored the Great Barrington Declaration in October 2020, which argued against lockdowns and movement restrictions during COVID. The declaration called for “focused protection” of the vulnerable while allowing low-risk populations to live normally.
Dr. Bhattacharya is now the senior official carrying out the duties of the CDC director and signing an order that restricts the movement of non-citizens based on a disease that, by the order’s own account, is not transmissible by the people it targets during the period it concerns.
Containing Ebola at the source costs less than banning travelers at the border.
The United States has responded to Ebola outbreaks before, and the tools that work are known. Exit screening in affected countries identifies symptomatic travelers before they board planes. Entry screening and 21-day monitoring at U.S. ports of entry catch cases that develop after arrival. Hospital preparedness — the thing that failed in Dallas in 2014 — ensures that when a patient presents with fever and a travel history, they are isolated, not sent home.
The economics tell the story. During the 2014 outbreak, the U.S. spent $5.4 billion on the international response — ending a 28,000-case epidemic across three countries, building lab and surveillance capacity in multiple countries, and creating the infrastructure that helped detect and contain subsequent outbreaks faster. All told, the U.S. spent an estimated $3.32 billion on direct funding, personnel deployment, and preparation and treatment of patients, and absorbed over $2 billion in economic losses and more than 10,000 jobs tied to exports — to manage four Ebola cases diagnosed on U.S. soil. Treating a single Ebola patient in a U.S. biocontainment unit cost up to $500,000. The global economic damage from an outbreak that was allowed to grow before the international response ramped up reached an estimated $53 billion.