

A New Era for Breast Cancer Screening
Can risk-based mammograms deliver the same protection with fewer harms?

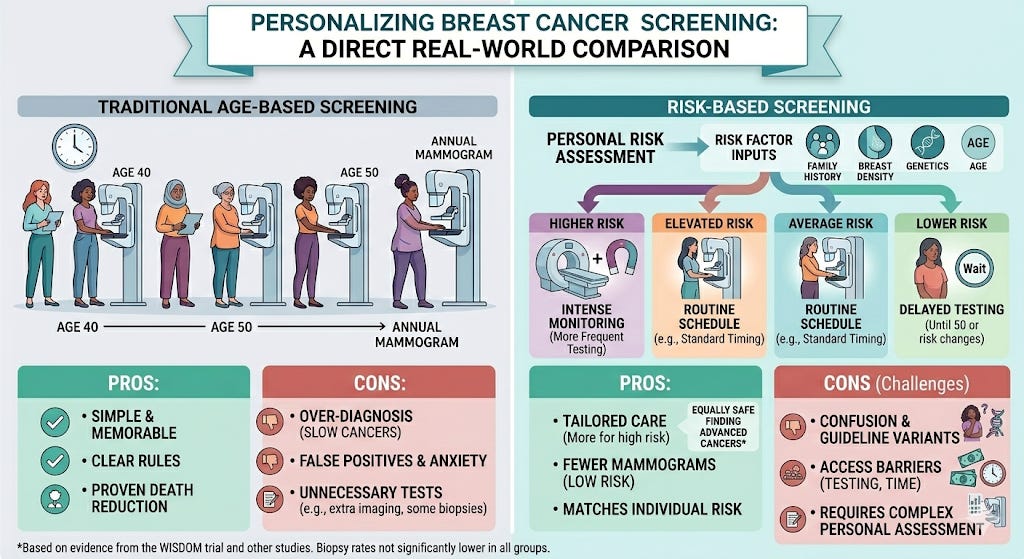
Matching breast cancer screening to risk
For decades, many women in the United States have followed a simple rule: start getting a mammogram at age 50 (and more recently, at age 40) and repeat it every year. The message was clear and easy to remember. But medicine is starting to ask a harder question: What if not every woman needs the same screening schedule?
Breast cancer is the most commonly diagnosed cancer among women in the U.S. In 2026, experts estimate that over 320 thousand women will be newly diagnosed with invasive breast cancer, and more than 42 thousand will die from it. The average woman faces about a 1 in 8 lifetime risk of developing breast cancer. Screening can help find cancer early, when it is easier to treat. But screening also has downsides, including false alarms and unnecessary biopsies. A major national study, known as the WISDOM trial, tested whether tailoring screening to a woman’s personal risk could be just as safe as annual mammograms. The results are helping reshape the debate over how often women should be screened.
How yearly mammograms became standard
Mammograms came into wide use starting in the 1970s. Over time, studies showed that screening could lower the risk of dying from breast cancer. As a result, many guidelines recommended regular mammograms based mainly on age.
Age-based screening is simple. Breast cancer risk rises as women get older.
But age is only one piece of the puzzle. Two women who are both 45 years old can have very different risks. One may have a strong family history of breast cancer or carry certain genetic changes. Another may have no known risk factors at all. Yet under annual screening rules, both women would get the same test at the same frequency.
Screening also has harms. Mammograms can find spots that look suspicious but are not cancer. These “false positives” can lead to stress, extra imaging, and biopsies. Screening can also lead to over-diagnosis: detecting slow-growing cancers that might never cause harm during a woman’s lifetime.
A personalized approach to mammograms
Risk-based screening tries to match the intensity of screening to a woman’s personal risk of developing breast cancer.
Doctors can estimate risk using models that include factors such as age, family history, breast density, and certain genetic variants. In the WISDOM trial, researchers used a detailed risk model that combined clinical information with genetic testing.
Women in the study were placed into four risk groups. Those at the highest risk were advised to have mammograms and breast MRI scans every six months, alternating between the two. Women at elevated risk were advised to get annual mammograms starting at age 40. Women at average risk were advised to get mammograms every two years starting at age 50. The lowest-risk women under age 50 were advised to delay screening until their risk increased or they turned 50.
The goal was simple: provide more screening to women most likely to benefit and less to those least likely to benefit.
Is risk-based screening safe?
The WISDOM trial included more than 28,000 women ages 40 to 74 from across the United States. They were randomly assigned to either annual screening or risk-based screening. Researchers followed them for a median of just over five years.
The main question was safety: would risk-based screening miss dangerous cancers?
The answer: risk-based screening was “non-inferior” to annual screening. In simple terms, it was just as safe as annual screening in detecting more advanced cancers.
However, one hoped-for benefit did not clearly appear. Researchers expected fewer biopsies in the risk-based group, but biopsy rates were not significantly lower. But women in the risk-based group had fewer mammograms, especially among women at lower risk of breast cancer.
Can personalized screening work in real life?
Even though the results are promising, experts say there are challenges.
In the WISDOM trial, many women did not strictly follow the screening schedule they were assigned. Some women in the yearly screening group got extra imaging. Some women in the high-risk group did not get as much MRI screening as recommended. When screening does not happen the way it was designed, it becomes harder to judge how well a new approach truly works.
There is also a bigger issue. When screening recommendations are not clear or consistent, confusion can grow. If different groups recommend different starting ages or different schedules, doctors and patients may not know which advice to follow. In busy clinics, complicated rules can lead to missed conversations about risk. Some women may be told to wait. Others may assume they are not at risk. Over time, people can fall through the cracks.
Personalized screening depends on knowing a woman’s risk. That often requires detailed questionnaires, breast density information, and sometimes genetic testing. Not all women have equal access to these tools. Women with less access to health care, less time off work, or less insurance coverage may be less likely to complete risk testing. If personalized screening is not built into routine care, it may widen gaps rather than close them.
Still, the trial shows that personalized screening can be done on a large scale. Researchers mailed genetic testing kits to women across all 50 states and successfully used those results to guide screening recommendations. The next challenge is making sure that any new system is simple, consistent, and easy to follow so that no one is left out.
The future of mammograms
The debate over annual versus risk-based screening is not about whether mammograms matter. They do. Screening has helped reduce deaths from breast cancer over time.
The real question is how to get the most benefit with the least harm.
Risk-based screening recognizes that women are not all the same. A woman at very high risk may benefit from more intensive screening, including MRIs. A woman at very low risk may safely wait longer between mammograms.
For now, national guidelines still vary, and annual screening remains common. But studies like WISDOM suggest that the future of breast cancer screening may be more personal, more precise, and more focused on matching care to each woman’s unique risk.
Esserman LJ, Fiscalini AS, Naeim A, et al. Risk-Based vs Annual Breast Cancer Screening: The WISDOM Randomized Clinical Trial. JAMA. 2026;335(9):763–774.
Baxter NN, Phillips KA. Unlocking the Potential of Risk-Based Screening for Breast Cancer: From Detection to Prevention. JAMA. 2026;335(9):758–760.
Keating NL, Pace LE. Risk-Based Screening for Breast Cancer: Time to Focus on Implementation. JAMA Oncol. Published online February 26, 2026.